Hyperparathyroidis
Hyperparathyroidis
m
m
Sarah Rodriguez, MD
Sarah Rodriguez, MD
Shawn Newlands, MD, PhD
Shawn Newlands, MD, PhD
University of Texas Medical Branch
University of Texas Medical Branch
Grand Rounds Presentation
Grand Rounds Presentation
February 2006
February 2006
PTH/Calcium Homeostasis
PTH/Calcium Homeostasis
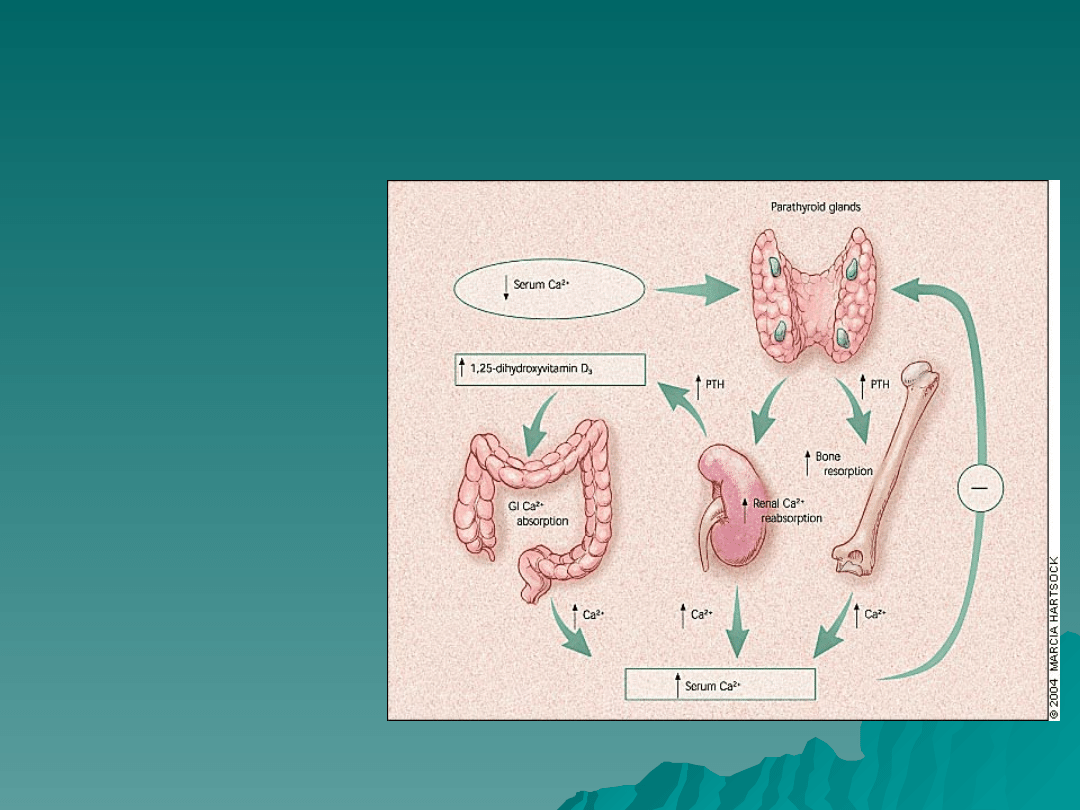
Low circulating serum
Low circulating serum
calcium
calcium
concentrations
concentrations
stimulate the
stimulate the
parathyroid glands to
parathyroid glands to
secrete PTH, which
secrete PTH, which
mobilizes calcium
mobilizes calcium
from bones by
from bones by
osteoclastic
osteoclastic
stimulation. PTH also
stimulation. PTH also
stimulates the
stimulates the
kidneys to reabsorb
kidneys to reabsorb
calcium and to
calcium and to
convert 25-
convert 25-
hydroxyvitamin D3
hydroxyvitamin D3
(produced in the
(produced in the
liver) to the active
liver) to the active
form,
form,
1,25-
1,25-
dihydroxyvitamin D3,
dihydroxyvitamin D3,
which stimulates GI
which stimulates GI
calcium absorption.
calcium absorption.
High serum calcium
High serum calcium
concentrations have a
concentrations have a
negative feedback
negative feedback
effect on PTH
effect on PTH
secretion.
secretion.
PTH
PTH
Renal effects (steady state maintenance)
Renal effects (steady state maintenance)
–
Inhibition of phosphate transport
Inhibition of phosphate transport
–
Increased reabsorption of calcium
Increased reabsorption of calcium
–
Stimulation of 25(OH)D-1alpha-hydroxylase
Stimulation of 25(OH)D-1alpha-hydroxylase
Bone effects (immediate control of blood Ca)
Bone effects (immediate control of blood Ca)
–
Causes calcium bone release within minutes
Causes calcium bone release within minutes
–
Chronic elevation increases bone remodeling and
Chronic elevation increases bone remodeling and
increased osteoclast-mediated bone resorption
increased osteoclast-mediated bone resorption
–
However, PTH administered intermittently
However, PTH administered intermittently
has been shown to increase bone formation
has been shown to increase bone formation
and this is a potential new therapy for
and this is a potential new therapy for
osteoporosis
osteoporosis
Hypercalcemia
Hypercalcemia
I.Parathyroid-related
I.Parathyroid-related
-Primary hyperparathyroidism
-Primary hyperparathyroidism
-Lithium therapy
-Lithium therapy
-Familial hypocalciuric hypercalcemia
-Familial hypocalciuric hypercalcemia
II. Malignancy-related
II. Malignancy-related
-Solid tumor with metastases (breast)
-Solid tumor with metastases (breast)
-Solid tumor with humoral mediation of hypercalcemia (lung, kidney)
-Solid tumor with humoral mediation of hypercalcemia (lung, kidney)
-Hematologic malignancies (multiple myeloma, lymphoma, leukemia)
-Hematologic malignancies (multiple myeloma, lymphoma, leukemia)
III. Vitamin D-related
III. Vitamin D-related
-Vitamin D intoxication
-Vitamin D intoxication
-↑ 1,25(OH)2D; sarcoidosis and other granulomatous diseases
-↑ 1,25(OH)2D; sarcoidosis and other granulomatous diseases
-Idiopathic hypercalcemia of infancy
-Idiopathic hypercalcemia of infancy
IV. Associated with high bone turnover
IV. Associated with high bone turnover
-Hyperthyroidism
-Hyperthyroidism
-Immobilization
-Immobilization
-Thiazides
-Thiazides
-Vitamin A intoxication
-Vitamin A intoxication
V. Associated with renal failure
V. Associated with renal failure
-Severe secondary hyperparathyroidism
-Severe secondary hyperparathyroidism
-Aluminum intoxication
-Aluminum intoxication
-Milk-alkali syndrome
-Milk-alkali syndrome
**Primary
hyperparathyroidis
m and cancer
account for 90% of
cases of
hypercalcemia
Primary
Primary
Hyperparathyroidism
Hyperparathyroidism
Estimated incidence is 1 case per 1000 men and 2-
Estimated incidence is 1 case per 1000 men and 2-
3 cases per 1000 women
3 cases per 1000 women
–
Incidence increases above age 40
Incidence increases above age 40
–
Most patients with sporadic primary
Most patients with sporadic primary
hyperparathyroidism are postmenopausal
hyperparathyroidism are postmenopausal
women with an average age of 55 years
women with an average age of 55 years
>80% of cases are caused by a solitary parathyroid
>80% of cases are caused by a solitary parathyroid
adenoma
adenoma
Approximately 10% are caused by “double
Approximately 10% are caused by “double
adenoma”
adenoma”
Primary HPT: Clinical
Primary HPT: Clinical
Features
Features
Symptomatic:
Symptomatic:
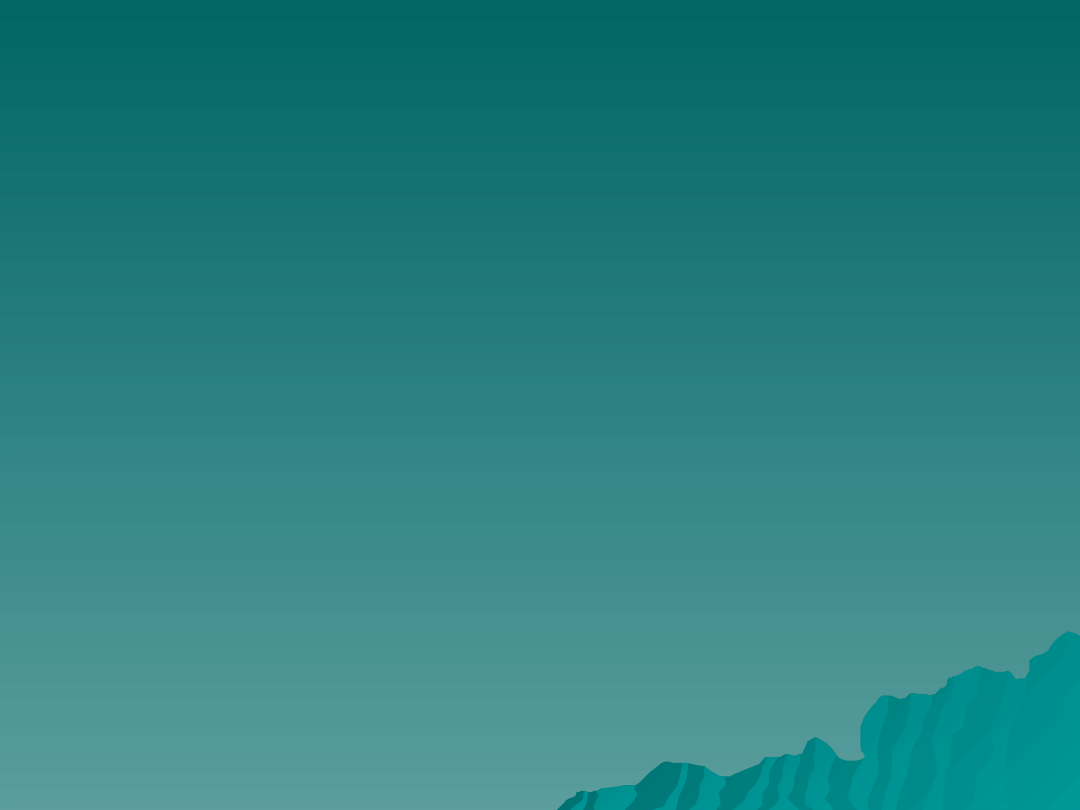
–
Osteitis fibrosa cystica
Osteitis fibrosa cystica
–
Nephrolithiasis
Nephrolithiasis
–
Pathologic fractures
Pathologic fractures
–
Neuromuscular disease
Neuromuscular disease
–
Life-threatening
Life-threatening
hypercalcemia
hypercalcemia
–
?Peptic Ulcer Disease
?Peptic Ulcer Disease
?Asymptomatic:
?Asymptomatic:
–
Fatigue
Fatigue
–
Subjective muscle weakness
Subjective muscle weakness
–
Depression
Depression
–
Increased thirst
Increased thirst
–
Polyuria
Polyuria
–
Constipation
Constipation
–
Musculoskeletal aches and
Musculoskeletal aches and
pains
pains

Work-Up
Work-Up
Intact PTH and chemistry panel
Intact PTH and chemistry panel
–
PTH elevated despite elevated serum calcium
PTH elevated despite elevated serum calcium
–
Serum phosphate in the low-normal to mildly decreased range
Serum phosphate in the low-normal to mildly decreased range
–
Look at the serum creatinine to evaluate for CRI/CRF
Look at the serum creatinine to evaluate for CRI/CRF
Rule out lithium or thiazide use
Rule out lithium or thiazide use
24-hour urine calcium excretion
24-hour urine calcium excretion
–
Used to rule out familial hypocalciuric hypercalcemia
Used to rule out familial hypocalciuric hypercalcemia
–
Values below 100mg/24 hours or a calcium creatinine
Values below 100mg/24 hours or a calcium creatinine
clearance ratio of <0.01 are suggestive of FHH
clearance ratio of <0.01 are suggestive of FHH
Wrist, spine and hip DEXA
Wrist, spine and hip DEXA
Consider KUB, IVP or CT to evaluate for kidney stones
Consider KUB, IVP or CT to evaluate for kidney stones
Ionized calcium versus serum calcium—the debate rages
Ionized calcium versus serum calcium—the debate rages
on….
on….
–
CORRECTED SERUM CALCIUM
CORRECTED SERUM CALCIUM
Serum calcium (mg/dL)+(0.8X[4-albumin (g/dL)])
Serum calcium (mg/dL)+(0.8X[4-albumin (g/dL)])
CA/CRT ratio: (24 hr
urine calciumXserum
crt)/(24 hr urine
crtXserum calcium)
Surgical Candidacy
Surgical Candidacy
Symptomatic primary HPT
Symptomatic primary HPT
NIH Consensus Development Panel 2002 Revised
NIH Consensus Development Panel 2002 Revised
Guidelines [if any of the following are met]
Guidelines [if any of the following are met]
–
Serum calcium greater than 1mg/dL above the upper
Serum calcium greater than 1mg/dL above the upper
limit of the reference range
limit of the reference range
–
24 hour urine calcium greater than 400 mg
24 hour urine calcium greater than 400 mg
–
Creatinine clearance reduced by more than 30%
Creatinine clearance reduced by more than 30%
compared with age-matched subjects
compared with age-matched subjects
–
Bone density at the lumbar spine, hip, or distal radius
Bone density at the lumbar spine, hip, or distal radius
more than 2.5 SD below peak bone mass
more than 2.5 SD below peak bone mass
–
Age under 50
Age under 50
–
Patients for whom medical surveillance is not desirable
Patients for whom medical surveillance is not desirable
or possible
or possible
creatinine clearance (mL/min) =
creatinine clearance (mL/min) =
((urine creatinine in mg/dL) * (urine
((urine creatinine in mg/dL) * (urine
volume in mL)) / ((plasma creatinine
volume in mL)) / ((plasma creatinine
in mg/dL) * (time period in minutes))
in mg/dL) * (time period in minutes))
Other Considerations in
Other Considerations in
Surgical Referral
Surgical Referral
Neuropsychological abnormalities
Neuropsychological abnormalities
–
Several studies document improvement in HRQL after
Several studies document improvement in HRQL after
parathroidectomy
parathroidectomy
–
Studies on neurobehavioral abnormalities have reported less
Studies on neurobehavioral abnormalities have reported less
consistent results with parathyroidectomy
consistent results with parathyroidectomy
Cardiovascular abnormalities
Cardiovascular abnormalities
–
Symptomatic patients suffer from increased cardiovascular
Symptomatic patients suffer from increased cardiovascular
mortality before and after treatment
mortality before and after treatment
–
Asymptomatic primary HPT is associated with LVH; some
Asymptomatic primary HPT is associated with LVH; some
studies suggest this is reversible with parathyroidectomy
studies suggest this is reversible with parathyroidectomy
–
Primary HPT patients have increased calcifications of mitral
Primary HPT patients have increased calcifications of mitral
and aortic valve
and aortic valve
Perimenopausal women
Perimenopausal women
–
Asymptomatic primary HPT associated with increased bone
Asymptomatic primary HPT associated with increased bone
turnover, reduced bone mineral density and higher risk for
turnover, reduced bone mineral density and higher risk for
fractures
fractures

Pre-Operative Imaging
Pre-Operative Imaging
High-resolution ultrasound
High-resolution ultrasound
–
Sensitivity 65-85% for adenoma; 30-90% for enlarged gland
Sensitivity 65-85% for adenoma; 30-90% for enlarged gland
–
Results suboptimal in pts with multinodular thyroid disease,
Results suboptimal in pts with multinodular thyroid disease,
pts with short thick neck, ectopic glands (15-20%)
pts with short thick neck, ectopic glands (15-20%)
–
May be useful in detecting sestamibi scan negative adenomas
May be useful in detecting sestamibi scan negative adenomas
CT with contrast/thin section
CT with contrast/thin section
–
Sensitivity of 46-87%
Sensitivity of 46-87%
–
Good for ectopic glands in the chest
Good for ectopic glands in the chest
MRI
MRI
–
Sensitivity of 65-80%
Sensitivity of 65-80%
–
Good for ectopic glands
Good for ectopic glands
Sestamibi
Sestamibi
–
85-95% accurate in localizing adenoma in primary HPT
85-95% accurate in localizing adenoma in primary HPT
Sestamibi-SPECT
Sestamibi-SPECT
–
Sensitivity 60% for enlarged gland and 98% for solitary
Sensitivity 60% for enlarged gland and 98% for solitary
adenomas
adenomas
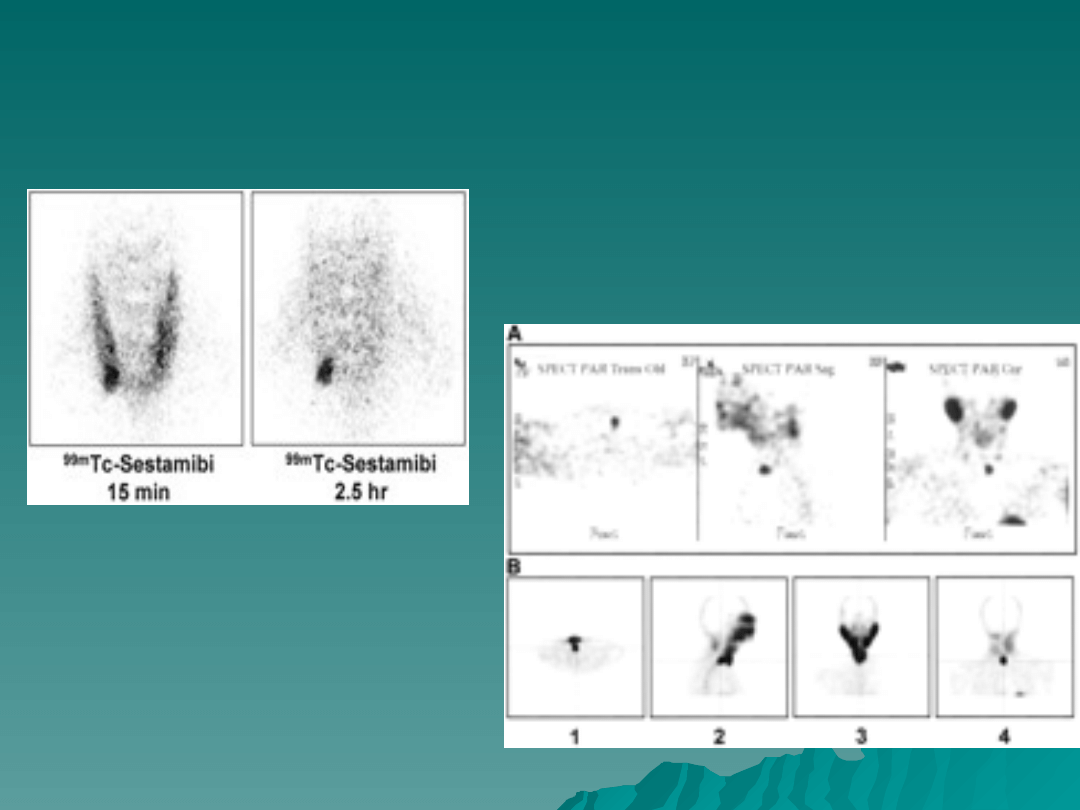
Scintigraphy Images
Traditional Sestamibi
Sestamibi-SPECT
Medical Management
Medical Management
Asymptomatic patients may elect to be
Asymptomatic patients may elect to be
closely followed and managed medically
closely followed and managed medically
–
A recent study of pts with asymptomatic primary
A recent study of pts with asymptomatic primary
HPT showed that the majority of pts followed for
HPT showed that the majority of pts followed for
ten years did not demonstrate an increase in
ten years did not demonstrate an increase in
serum calcium or PTH levels—25% of patients
serum calcium or PTH levels—25% of patients
had progressive disease including worsening
had progressive disease including worsening
hypercalcemia, hypercalciuria and reduction in
hypercalcemia, hypercalciuria and reduction in
bone mass—younger patients more likely to have
bone mass—younger patients more likely to have
progression of disease
progression of disease
Patients opting not to have surgery should
Patients opting not to have surgery should
have a serum calcium level drawn every 6
have a serum calcium level drawn every 6
months and should have annual bone
months and should have annual bone
densiometry at all three sites
densiometry at all three sites

Medical Management Primary
Medical Management Primary
HPT
HPT
Estrogen
Estrogen
–
Dose required is high
Dose required is high
SERMs
SERMs
–
Reduction in serum calcium and markers of
Reduction in serum calcium and markers of
bone turnover after 4 weeks
bone turnover after 4 weeks
Bisphosphonates
Bisphosphonates
–
Studies have shown increase in lumbar spine
Studies have shown increase in lumbar spine
and femoral neck mineral density
and femoral neck mineral density
Calcium/Vitamin D
Calcium/Vitamin D
Calcimimetic agents (Cinacalcet)
Calcimimetic agents (Cinacalcet)
–
Under investigation for primary HPT
Under investigation for primary HPT
Familial Syndromes
Familial Syndromes
MEN I
MEN I
MEN IIA
MEN IIA
Familial Hypocalciuric Hypercalcemia
Familial Hypocalciuric Hypercalcemia
Hyperparathyroidism-jaw tumor
Hyperparathyroidism-jaw tumor
syndrome
syndrome
–
Fibro-osseous jaw tumors
Fibro-osseous jaw tumors
–
Renal cysts
Renal cysts
–
Solid renal tumors
Solid renal tumors
Familial isolated hyperparathyroidism
Familial isolated hyperparathyroidism

MEN I
MEN I
MEN I
MEN I
–
1 in 30,000 persons
1 in 30,000 persons
–
Features:
Features:
Hyperparathyroidism (95%)
Hyperparathyroidism (95%)
–
Most common and earliest endocrine manifestation
Most common and earliest endocrine manifestation
Gastrinoma (45%)
Gastrinoma (45%)
Pituitary tumor (25%)
Pituitary tumor (25%)
Facial angiofibroma (85%)
Facial angiofibroma (85%)
Collagenoma (70%)
Collagenoma (70%)
HPT in MEN I
HPT in MEN I
–
Early onset
Early onset
–
Multiple glands affected
Multiple glands affected
–
Post-op hypoparathyroidism more common (more
Post-op hypoparathyroidism more common (more
extensive surgery)
extensive surgery)
–
Successful subtotal parathyroidectomy followed by
Successful subtotal parathyroidectomy followed by
recurrent HPT in 10 years in 50% of cases
recurrent HPT in 10 years in 50% of cases
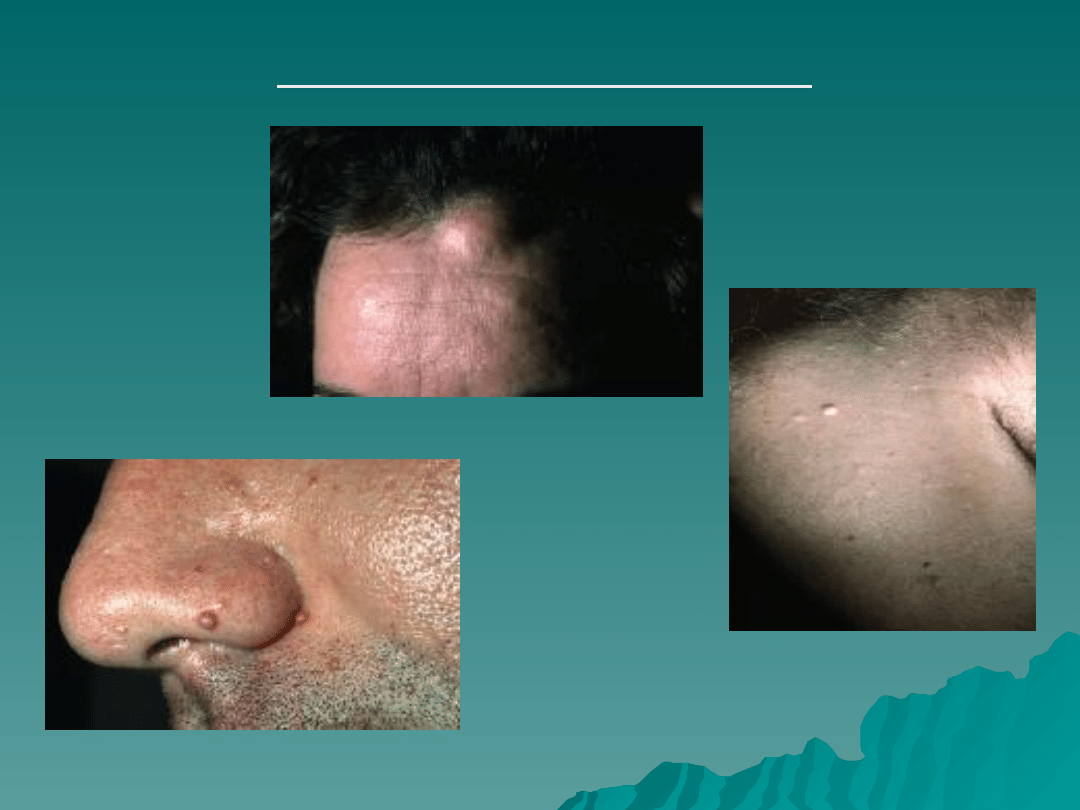
STIGMATA OF MEN I
Lipoma
s
Collagenomas
Angiofibromas

MEN IIA (Sipple’s Syndrome)
MEN IIA (Sipple’s Syndrome)
Features:
Features:
–
MTC(95%)
MTC(95%)
–
Pheochromocytoma(50%)
Pheochromocytoma(50%)
–
HPT(20%)
HPT(20%)
RET mutation (98%)
RET mutation (98%)
1 in 30,000-50,000 people
1 in 30,000-50,000 people
Usually single adenoma but may
Usually single adenoma but may
have multi-gland hyperplasia
have multi-gland hyperplasia
Familial Hypocalciuric
Familial Hypocalciuric
Hypercalcemia
Hypercalcemia
This benign condition can be easily mistaken for mild
This benign condition can be easily mistaken for mild
hyperparathyroidism. It is an autosomal dominant
hyperparathyroidism. It is an autosomal dominant
inherited disorder characterized by hypocalciuria
inherited disorder characterized by hypocalciuria
(usually < 50 mg/24 h), variable hypermagnesemia,
(usually < 50 mg/24 h), variable hypermagnesemia,
and normal or minimally elevated levels of PTH.
and normal or minimally elevated levels of PTH.
These patients do not normalize their hypercalcemia
These patients do not normalize their hypercalcemia
after subtotal parathyroid removal and should not be
after subtotal parathyroid removal and should not be
subjected to surgery. The condition has an excellent
subjected to surgery. The condition has an excellent
prognosis and is easily diagnosed with family history
prognosis and is easily diagnosed with family history
and urinary calcium clearance determination.
and urinary calcium clearance determination.

Secondary
Secondary
Hyperparathyroidism
Hyperparathyroidism
Decreased GFR leads to reduced inorganic phosphate
Decreased GFR leads to reduced inorganic phosphate
excretion and consequent phosphate retention
excretion and consequent phosphate retention
Retained phosphate has a direct stimulatory effect on PTH
Retained phosphate has a direct stimulatory effect on PTH
synthesis and on cellular mass of the parathyroid glands
synthesis and on cellular mass of the parathyroid glands
Retained phosphate also causes excessive production and
Retained phosphate also causes excessive production and
secretion of PTH through lowering of ionized Ca2+ and by
secretion of PTH through lowering of ionized Ca2+ and by
suppression of calcitriol production
suppression of calcitriol production
Reduced calcitriol production results both from decreased
Reduced calcitriol production results both from decreased
synthesis due to reduced kidney mass and from
synthesis due to reduced kidney mass and from
hyperphosphatemia.
hyperphosphatemia.
–
Low calcitriol levels, in turn, lead to hyperparathyroidism via
Low calcitriol levels, in turn, lead to hyperparathyroidism via
both direct and indirect mechanisms. Calcitriol is known to have
both direct and indirect mechanisms. Calcitriol is known to have
a direct suppressive effect on PTH transcription and therefore
a direct suppressive effect on PTH transcription and therefore
reduced calcitriol in CRD causes elevated levels of PTH
reduced calcitriol in CRD causes elevated levels of PTH
–
Reduced calcitriol leads to impaired Ca2+ absorption from the
Reduced calcitriol leads to impaired Ca2+ absorption from the
GI tract, thereby leading to hypocalcemia, which then increases
GI tract, thereby leading to hypocalcemia, which then increases
PTH secretion and production.
PTH secretion and production.
Secondary HPT
Secondary HPT
Clinical presentation
Clinical presentation
–
Usually asymptomatic
Usually asymptomatic
Diagnosis
Diagnosis
–
Elevated PTH in the setting of low or normal serum calcium is diagnostic
Elevated PTH in the setting of low or normal serum calcium is diagnostic
–
If phosphorous is elevated, cause is renal
If phosphorous is elevated, cause is renal
–
If phosphorous is low, other causes of vit D deficiency should be sought
If phosphorous is low, other causes of vit D deficiency should be sought
Prevention
Prevention
–
Vit D replacement
Vit D replacement
–
Phosphorus binders [Sevelamer]
Phosphorus binders [Sevelamer]
Treatment
Treatment
–
Medical
Medical
Calcimimetic agents
Calcimimetic agents
–
Surgical
Surgical
Considered in cases of refractory
Considered in cases of refractory
severe hypercalcemia, severe
severe hypercalcemia, severe
bone disease, severe pruritis,
bone disease, severe pruritis,
calciphylaxis, severe myopathy
calciphylaxis, severe myopathy
Tertiary
Tertiary
Hyperparathyroidism
Hyperparathyroidism
Tertiary hyperparathyroidism develops in patients with
Tertiary hyperparathyroidism develops in patients with
long-standing secondary hyperparathyroidism, which
long-standing secondary hyperparathyroidism, which
stimulates the growth of an autonomous adenoma. A
stimulates the growth of an autonomous adenoma. A
clue to the diagnosis of tertiary hyperparathyroidism is
clue to the diagnosis of tertiary hyperparathyroidism is
intractable hypercalcemia and/or an inability to control
intractable hypercalcemia and/or an inability to control
osteomalacia despite vitamin D therapy.
osteomalacia despite vitamin D therapy.
Surgical Referral
Surgical Referral
- calcium- phosphate product > 70
- calcium- phosphate product > 70
- severe bone disease and pain
- severe bone disease and pain
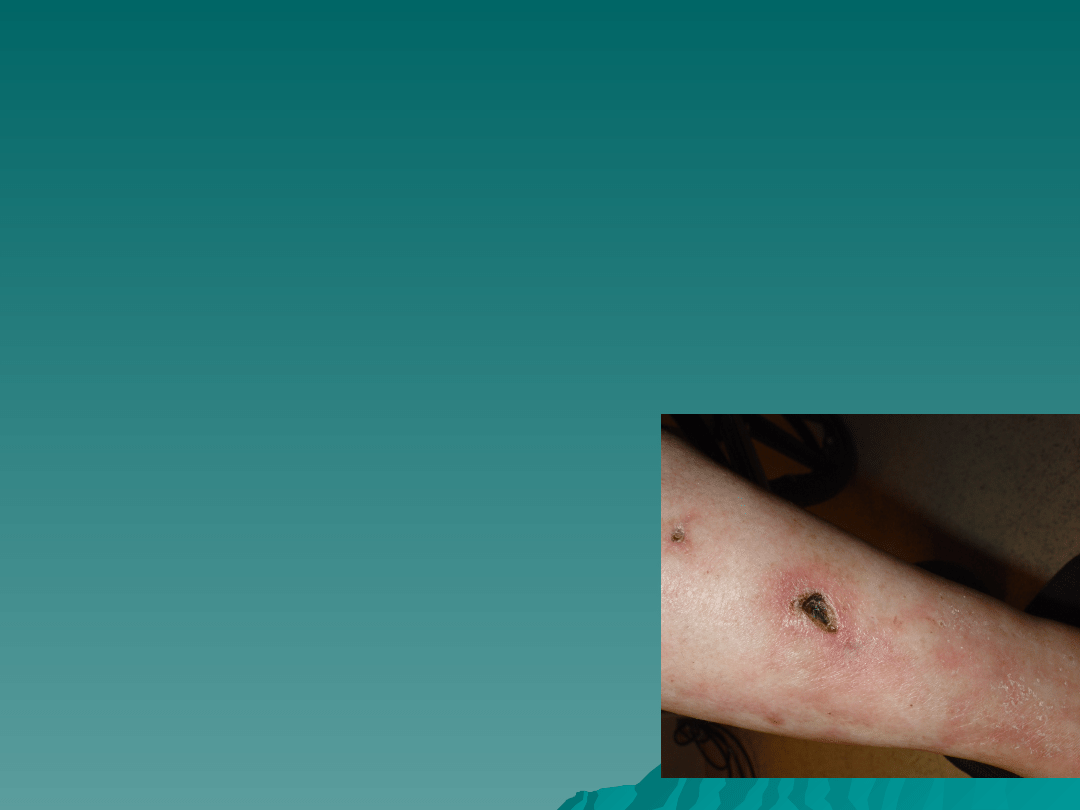
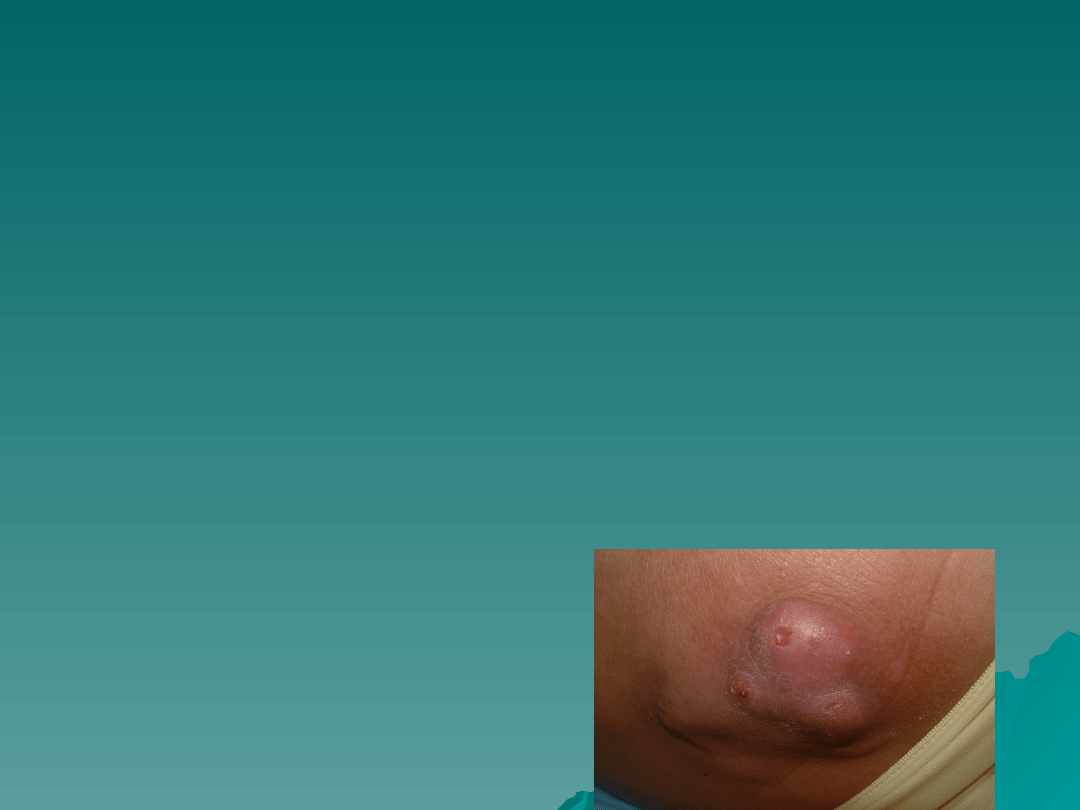
-intractable pruritus
-intractable pruritus
- extensive soft tissue calcification with tumoral calcinosis
- extensive soft tissue calcification with tumoral calcinosis
-calciphylaxis
-calciphylaxis
Lab Abnormalities
Lab Abnormalities
Primary HPT
Primary HPT
–
Increased serum calcium
Increased serum calcium
–
Phosphorus in low normal range
Phosphorus in low normal range
–
Urinary calcium elevated
Urinary calcium elevated
Secondary HPT (renal etiology)
Secondary HPT (renal etiology)
–
Low or normal serum calcium
Low or normal serum calcium
–
High phosphorus
High phosphorus
Tertiary HPT (renal etiology)
Tertiary HPT (renal etiology)
–
High calcium and phosphorus
High calcium and phosphorus

Quiz #1
Quiz #1
A 45 year old woman is referred to you for
A 45 year old woman is referred to you for
evaluation of elevated calcium and PTH
evaluation of elevated calcium and PTH
found on routine lab work. The PCP
found on routine lab work. The PCP
ordered a 24 hour urine collection and the
ordered a 24 hour urine collection and the
urinary calcium is less than 50 mg for 24
urinary calcium is less than 50 mg for 24
hrs. Next step?
hrs. Next step?
A. Order the mibi/schedule the surgery
A. Order the mibi/schedule the surgery
B. Consider estrogen replacement in this
B. Consider estrogen replacement in this
perimenopausal woman
perimenopausal woman
C. Take a careful family history
C. Take a careful family history
D. Look for stigmata of MEN I
D. Look for stigmata of MEN I
Quiz #2
Quiz #2
You receive a hospital consult for
You receive a hospital consult for
“parathyroidectomy”. You look at the pts
“parathyroidectomy”. You look at the pts
labs and note elevated PTH, calcium and
labs and note elevated PTH, calcium and
phosphorus.
phosphorus.
A. Have primary team order a mibi before you
A. Have primary team order a mibi before you
see the patient
see the patient
B. Suspect MEN IIA and have the primary team
B. Suspect MEN IIA and have the primary team
order ret-proto oncogene screening
order ret-proto oncogene screening
C. Evaluate the pt in the dialysis unit with careful
C. Evaluate the pt in the dialysis unit with careful
questioning as to symptoms of pruritis, skin
questioning as to symptoms of pruritis, skin
calcifications or necrosis
calcifications or necrosis
Quiz #3
Quiz #3
Primary HPT:
Primary HPT:
A.
A.
Is more common in post-menopausal
Is more common in post-menopausal
women
women
B.
B.
Is most likely due to a parathyroid
Is most likely due to a parathyroid
adenoma
adenoma
C.
C.
Usually is discovered when the pt is
Usually is discovered when the pt is
“asymptomatic”
“asymptomatic”
D.
D.
All of the above
All of the above

Quiz #4
Quiz #4
Surgical candidacy for primary HPT
Surgical candidacy for primary HPT
includes:
includes:
A.
A.
24 hour urine calcium greater than 400
24 hour urine calcium greater than 400
mg
mg
B.
B.
Age under 50
Age under 50
C.
C.
Creatinine clearance decreased 30%
Creatinine clearance decreased 30%
when compared to age matched norms
when compared to age matched norms
D.
D.
All of the above
All of the above

Quiz #5
Quiz #5
You are in endocrine multidisciplinary
You are in endocrine multidisciplinary
clinic presenting a patient. You are
clinic presenting a patient. You are
asked “What is the calcium-
asked “What is the calcium-
creatinine clearance ratio?”
creatinine clearance ratio?”
–
You reply “ask an endorinologist”
You reply “ask an endorinologist”
–
You ask “the calcium creatinine what?”
You ask “the calcium creatinine what?”
–
You say “Let me just answer this page,
You say “Let me just answer this page,
I’ll be right back” and you consult Dr.
I’ll be right back” and you consult Dr.
Quinn’s online textbook
Quinn’s online textbook
Quiz #6
Quiz #6
You have a patient with “asymptomatic”
You have a patient with “asymptomatic”
primary HPT. You discuss surgery with her
primary HPT. You discuss surgery with her
but she is very reluctant. You tell her that
but she is very reluctant. You tell her that
patients with primary HPT can be
patients with primary HPT can be
followed medically and…
followed medically and…
A.
A.
Her chance of dying from complications of
Her chance of dying from complications of
primary HPT in the next year are 50%
primary HPT in the next year are 50%
B.
B.
She will need monthly serum calcium and 24
She will need monthly serum calcium and 24
hour urine collections to monitor her disease
hour urine collections to monitor her disease
C.
C.
Most patients with asymptomatic primary
Most patients with asymptomatic primary
HPT do not demonstrate progression of their
HPT do not demonstrate progression of their
disease over a ten year period
disease over a ten year period
Document Outline
- Hyperparathyroidism
- PTH/Calcium Homeostasis
- PTH
- Hypercalcemia
- Primary Hyperparathyroidism
- Primary HPT: Clinical Features
- Work-Up
- Surgical Candidacy
- Other Considerations in Surgical Referral
- Pre-Operative Imaging
- Slide 11
- Medical Management
- Medical Management Primary HPT
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Familial Hypocalciuric Hypercalcemia
- Secondary Hyperparathyroidism
- Slide 20
- Tertiary Hyperparathyroidism
- Lab Abnormalities
- Quiz #1
- Quiz #2
- Quiz #3
- Quiz #4
- Quiz #5
- Quiz #6
Wyszukiwarka
Podobne podstrony:
Positron emission tomography slides
jj slides tex
credit slides 1
slides01
Thyroid benign slides
Criando Bons Slides
Munsell Slides
Chaos Deterministyczny p19 slides
Vision Slides
Criando Slides
lecture slides 05
F99 Carley slides
Electrocardiograms slides
hai burden slides notes 2002
ZW Pol pien PP 2011 2012 odcinek 1 dla studentów slides z wykładów w dniach 02 16 10 2011
lecture slides
więcej podobnych podstron