Risk of Cancer by ATM Missense Mutations in the
General Population
Sarah Louise Dombernowsky, Maren Weischer, Kristine Højgaard Allin, Stig Egil Bojesen,
Anne Tybjærg-Hansen, and Børge Grønne Nordestgaard
From the Department of Clinical
Biochemistry, Herlev University Hospi-
tal, Herlev; the Department of Clinical
Biochemistry, Rigshospitalet, Copenha-
gen University Hospital, and the Copen-
hagen City Heart Study, Bispebjerg
University Hospital, University of
Copenhagen, Denmark.
Submitted September 28, 2007;
accepted March 11, 2008.
B.G.N. was supported by the Danish
Medical Research Council, the Copen-
hagen County Foundation, and the
Danish Heart Foundation.
Authors’ disclosures of potential con-
flicts of interest and author contribu-
tions are found at the end of this
article.
Corresponding author: Børge G.
Nordestgaard, MD, DMSc, Department
of Clinical Biochemistry, Herlev Univer-
sity Hospital, Herlev Ringvej 75,
DK-2730 Herlev, Denmark; e-mail:
brno@heh.regionh.dk.
© 2008 by American Society of Clinical
Oncology
0732-183X/08/2618-3057/$20.00
DOI: 10.1200/JCO.2007.14.6613
A
B
S
T
R
A
C
T
Purpose
Truncating and missense mutations in the ATM gene, which cause insufficient DNA damage
surveillance, allow damaged cells to proceed into mitosis, which eventually results in increased
cancer susceptibility. We tested the hypotheses that ATM Ser49Cys and ATM Ser707Pro
heterozygosity increase the risk of cancer overall, of breast cancer, and of 26 other cancer
subtypes in the general population.
Patients and Methods
We genotyped 10,324 individuals from the Danish general population who were observed
prospectively for 36 years, during which 2,056 developed cancer.
Results
Multifactorially adjusted hazard ratios for ATM Ser49Cys heterozygotes versus noncarriers were
1.2 (95% CI, 0.9 to 1.5) for cancer overall, 0.8 (95% CI, 0.3 to 2.0) for breast cancer, 4.8 (95% CI,
2.2 to 11) for melanoma, 2.3 (95% CI, 1.1 to 5.0) for prostate cancer, and 3.4 (95% CI, 1.1 to 11)
for cancer of the oral cavity/pharynx. Multifactorially adjusted hazard ratios for ATM Ser707Pro
heterozygotes versus noncarriers were 0.8 (95% CI, 0.6 to 1.2) for cancer overall, 0.6 (95% CI, 0.2
to 1.6) for breast cancer, 10 (95% CI, 1.1 to 93) for thyroid/other endocrine tumors, and 2.7 (95%
CI, 1.0 to 7.6) for cancer of corpus uteri.
Conclusion
ATM missense mutations do not increase the risk of cancer overall or of breast cancer in the
general population; however, we observed in exploratory analyses that ATM missense
mutations may be associated with an increased risk of other cancer subtypes. As we did
multiple comparisons, some of these findings could represent chance findings rather than
real phenomena.
J Clin Oncol 26:3057-3062. © 2008 by American Society of Clinical Oncology
INTRODUCTION
ATM encodes the ataxia telangiectasia mutated pro-
tein, which is activated in response to DNA double-
strand breakage that is caused by especially ionizing
radiation.
1
When activated, ATM phosphorylates a
variety of downstream substrates, including p53,
CHEK2 and BRCA1, thereby mediating cell cycle
arrest, DNA repair, or apoptosis.
2
Insufficient DNA
damage surveillance by cell cycle checkpoints allows
damaged cells to proceed into mitosis, which even-
tually results in increased cancer susceptibility.
ATM dysfunction caused by homozygosity of
truncating and missense ATM mutations results in
the clinical condition called ataxia telangiectasia, in
which patients suffer neurologic symptoms and in-
creased cancer susceptibility.
3
Relatives of patients
with ataxia telangiectasia obligate heterozygous for a
broad range of truncating and missense ATM muta-
tions also have increased cancer susceptibility.
4,5
It
is, therefore, possible that ATM missense mutations
could increase the risk of sporadic cancer in the
general population.
3
So far, various missense mutations in ATM
have been associated with breast, lung, and prostate
cancer in case-control studies.
6-8
Among these,
ATM Ser49Cys and ATM Ser707Pro have been pre-
viously associated with two- to five-fold increased
risks of breast cancer in some,
8-10
but not all, stud-
ies.
11,12
ATM Ser49Cys is located in a region involved
in binding chromatin and p53,
13,14
and, therefore,
could alter the targeting of ATM to sites of DNA
damage. Furthermore, the introduction of cysteine
could possibly interfere with the formation of disul-
fide bridges. ATM Ser707Pro also is likely to interfere
with secondary and tertiary protein structure, as the
exchange of proline for serine introduces a much
bulkier side chain and removes a hydroxyl group
J
OURNAL OF
C
LINICAL
O
NCOLOGY
O R I G I N A L
R E P O R T
V O L U M E
2 6
䡠
N U M B E R
1 8
䡠
J U N E
2 0
2 0 0 8
© 2008 by American Society of Clinical Oncology
3057
that possibly participates in hydrogen bonding. Therefore, ATM
Ser49Cys and ATM Ser707Pro carriers could have impaired ATM
function and, thereby, have increased susceptibility to cancer.
We tested the hypotheses that ATM Ser49Cys and ATM
Ser707Pro heterozygosity increase the risk of cancer overall, of breast
cancer, and of 26 other cancer subtypes in the general population;
although the two former were primary hypotheses, the latter repre-
sents an exploratory analysis. For this purpose, we genotyped 10,324
individuals from the Danish general population who were observed
prospectively for 36 years, during which 2,056 developed a first cancer.
Homozygotes for these two mutations were too rare to reliably test
these hypotheses; however, we still report some results on homozy-
gotes for completion.
PATIENTS AND METHODS
Participants
We performed a population-based study of 10,324 individuals from the
Danish general population who were participating in the Copenhagen City
Heart Study, a prospective study. Participants were selected at random after
age and sex stratification on the basis of their unique Danish central person
registration numbers and were invited for a free health examination. Partici-
pants were interviewed in 1976 to 1978, 1981 to 1983, 1991 to 1994, and 2001
to 2003 regarding alcohol consumption, smoking habits, and reproductive
history (women only). Before each examination, participants filled out a
questionnaire, which was validated by an examiner at the day of attendance. At
each examination, height and weight were measured for a calculation of body
mass index (BMI). At the 1991 to 1994 and the 2001 to 2003 examinations,
blood samples for DNA extraction were drawn. Of the 17,600 individuals
invited to these two examinations, 10,324 (59%) participated and were geno-
typed for the present study. Roughly 99% of the participants were white and of
Danish descent. Diagnoses of invasive cancer (according to the WHO Inter-
national Classification of Diseases, seventh edition
15
) for the whole cohort
from 1947 through March 11, 2004, were obtained from the Danish Cancer
Registry, which identifies 98% of all cancers in Denmark.
16,17
According to WHO criteria, cancer diagnoses were divided in 27 sub-
groups
15
: oral cavity/pharynx (n
⫽ 35), esophagus (n ⫽ 23), stomach (n ⫽
29), colon/rectum/anus (n
⫽ 225), liver/biliary tract (n ⫽ 36), pancreas (n ⫽
50), larynx (n
⫽ 30), lung (n ⫽ 247), melanoma (n ⫽ 66), breast (n ⫽ 294),
cervix uteri (n
⫽39),corpusuteri(n⫽80),ovary(n⫽53),prostate(n⫽123),
testis (n
⫽ 10), bladder/excretory urinary tract (n ⫽ 158), kidney (n ⫽ 33),
brain/nervous tissue (n
⫽ 40), thyroid/other endocrine tumors (n ⫽ 5),
non-Hodgkin’s lymphoma (n
⫽ 39), Hodgkin’s disease (n ⫽ 4), multiple
myeloma (n
⫽ 20), leukemia (n ⫽ 53), nonmelanoma skin (n ⫽ 509),
sarcoma/other mesodermal tumors (n
⫽ 19), other tumors (n ⫽ 34), and
metastases (n
⫽ 39). Among study participants, 2,056 had a first cancer during
follow-up. In total, we detected 2,293 cancers, of which 237 occurred in
participants who had previously had another cancer.
Follow-up time for each participant began at the establishment of the
Danish Civil Register System (April 1, 1968) or on the participant’s 20th
birthday, whichever came last. Follow-up ended at death, at event, at emigra-
tion, or on March 11, 2004, whichever came first. Participants with cancer
before their 20th birthday or April 1, 1968, were excluded (n
⫽ 70). Only
participants successfully genotyped for both ATM Ser49Cys and ATM
Ser707Pro were included. Maximum and median follow-up periods were 36
and 27 years, respectively. Follow-up was 100% complete.
Genotyping
Genotyping of ATM Ser49Cys and ATM Ser707Pro was done on isolated
leukocyte DNA using TaqMan assays (Applied Biosystems, Foster City, CA).
Primers and probes are available from the authors on request. In each 384-well
plate, two known heterozygotes and one known homozygote were run as
positive controls, and water was run as a negative control. To reduce the
number of no-calls to a minimum, two rounds of reruns were performed.
Ethics
All participants gave written informed consent. Herlev University Hos-
pital and the Danish ethical committee for Copenhagen and Frederiksberg
approved the study (No. 100.2039/91).
Statistical Analyses
We used the statistical software STATA (STATA Corp, College Station,
TX). Two-sided P
⬍ .05 was regarded as significant. Statistical tests used were
the Mann-Whitney U test, the Pearson
2
test, the log-rank test, and Cox
regression with delayed entry and age as the underlying time variable; thus,
analysis is automatically adjusted for age. Multifactorially adjusted models
included time-dependent covariates from the 1976 to 1978, 1981 to 1983, 1991
to 1994, and 2001 to 2003 examinations. This implies that, initially, baseline
covariate values were used for the following years until that person was exam-
ined again, after which the new value was used in the analyses. If only baseline
values were available, these were used for adjustment during the entire
follow-up period. To analyze the overall cancer risk, multifactorial adjustment
included age, sex, BMI (
ⱕ 25 kg/m
2
v
⬎ 25 kg/m
2
to
ⱕ 30 kg/m
2
v
⬎ 30
kg/m
2
), weekly alcohol intake (0 g/wk v 1 to 168 g/wk v
⬎168g/wkforwomen,
and 0 g/wk v 1 to 252 g/wk v
⬎ 252 g/wk for men), present smoking status (yes
v no), smoking history (ever v never), and—additionally for women—parity
(number of children), nulliparity (yes v no), use of oral contraceptive drugs at
the time of examination (yes v no), menopausal status (premenopausal v
postmenopausal), and use of hormonal replacement therapy at the time of
examination (yes v no). The proportional hazard assumption for Cox regres-
sion was tested graphically by plotting ln(
⫺ln[survival probability]) versus
ln(analysis time) for all comparisons; no violations were observed. Two-factor
interaction terms between each of the two genotypes and each of the covariates
listed above were tested for interaction in the Cox regression. Population
attributable risk was estimated as (f[HR
⫺ 1]) ⫼ (1 ⫹ f[HR ⫺ 1]), in which f
is the frequency of ATM Ser49Cys or ATM Ser707Pro in the population and
HR is the corresponding hazard ratio for cancer.
18
RESULTS
We were able to genotype for both ATM Ser49Cys and ATM Ser707Pro
in 10,317 of 10,324 included participants, which corresponds to a call
rate of 99.9%. Of those genotyped, 0.02% were homozygotes, 2.5%
were heterozygotes, and 97.5% were noncarriers of ATM Ser49Cys;
0.01% were homozygotes, 2.1% were heterozygotes, and 97.9% were
noncarriers of ATM Ser707Pro. Both distributions were in Hardy-
Weinberg equilibrium (ATM Ser49Cys, P
⫽ .77; ATM Ser707Pro,
P
⫽ .87 by
2
test). Because of the small number of homozygotes, we
only calculated hazard ratios for heterozygotes versus noncarriers.
There were two ATM Ser49Cys homozygotes: both were female, and
one of these developed breast cancer. There was one ATM Ser707Pro
homozygote: this participant was male and did not develop any can-
cer. Table 1 lists characteristics of participants at study entry. We
detected 2,056 participants with a first cancer during the 36 years
of follow-up.
Risk of Any Cancer by ATM Ser49Cys
Cancer incidences for the combined sexes were 67 per 10,000
person-years for ATM Ser49Cys noncarriers and 79 for heterozygotes
(Table 2). The multifactorially adjusted hazard ratio of developing any
cancer in ATM Ser49Cys heterozygotes versus noncarriers was 1.2
(95% CI, 0.9 to 1.5) for the sexes combined, 1.0 (95% CI, 0.7 to 1.5) for
women, and 1.4 (95% CI, 0.9 to 2.0) for men. None of the covariates
listed in Table 1 interacted with the ATM Ser49Cys genotype on the
risk of cancer.
Dombernowsky et al
3058
© 2008 by American Society of Clinical Oncology
J
OURNAL OF
C
LINICAL
O
NCOLOGY
Risk of Breast Cancer and Other Cancer Subtypes by
ATM Ser49Cys
The incidence of breast cancer in women per 10,000 person-years
was 17 for ATM Ser49Cys noncarriers and 17 for heterozygotes (Table
3). The multifactorially adjusted hazard ratio for heterozygotes versus
noncarriers was 0.8 (95% CI, 0.3 to 2.0).
In exploratory analyses among 26 other cancer subtypes, we
found ATM Ser49Cys heterozygosity to be associated with melanoma,
prostate cancer, and cancer of the oral cavity/pharynx (Table 3). The
multifactorially adjusted hazard ratio in ATM Ser49Cys heterozygotes
versus noncarriers was 4.8 (95% CI, 2.2 to 11) for melanoma, 2.3 (95%
CI, 1.1 to 5.0) for prostate cancer, and 3.4 (95% CI, 1.1 to 11) for
cancer of the oral cavity/pharynx. However, these risk estimates were
based on only seven heterozygotes with melanoma, seven heterozy-
gotes with prostate cancer, and three heterozygotes with cancer of the
oral cavity/pharynx.
Risk of Any Cancer by ATM Ser707Pro
Cancer incidence for the combined sexes was 67 per 10,000
person-years for both noncarriers and heterozygotes (Table 2). The
multifactorially adjusted hazard ratio for heterozygotes versus non-
carriers was 0.8 (95% CI, 0.6 to 1.2) for sexes combined, 0.8 (95% CI,
0.5 to 1.3) for women, and 0.8 (95% CI, 0.5 to 1.3) for men. None of
the covariates listed in Table 1 interacted with the ATM Ser707Pro
genotype on the risk of cancer.
Risk of Breast Cancer and Other Cancer Subtypes by
ATM Ser707Pro
The incidence of breast cancer in women per 10,000 person-years
was 17 and 10 for noncarriers and heterozygotes, respectively (Table
3). The multifactorially adjusted hazard ratio of developing breast
cancer in women who were ATM Ser707Pro heterozygotes versus
noncarriers was 0.6 (95% CI, 0.2 to 1.6).
In exploratory analyses among 26 other cancer subtypes, we
found ATM Ser707Pro heterozygosity to be associated with thyroid/
other endocrine tumors and cancer of corpus uteri (Table 3). The
multifactorially adjusted hazard ratio in ATM Ser707Pro heterozy-
gotes versus noncarriers was 10 (95% CI, 1.1 to 93) for thyroid/other
endocrine tumors, and 2.7 (95% CI, 1.0 to 7.6) for cancer of corpus
uteri. However, these risk estimates were based on only one heterozy-
gote with thyroid/other endocrine tumors and five heterozygotes with
cancer of corpus uteri.
DISCUSSION
An association between ATM mutation heterozygosity and an in-
creased risk of cancer was first suspected when several studies reported
an increased risk of cancer, particularly breast cancer, in relatives of
patients with ataxia telangiectasia.
4,5
Since then, a multitude of studies
have evaluated numerous ATM mutations, most often in the setting of
small, case-control studies, with varying results.
6-12,19
The present
paper is the first to examine ATM missense mutation heterozygosity in
a prospective study of the general population with respect to the risk
of cancer.
Our findings in the general population of no increased overall
risk of cancer in ATM Ser49Cys and ATM Ser707Pro heterozygotes
compared with noncarriers could seem to contrast with the increased
risk of cancer overall observed in obligate heterozygous ataxia telangi-
ectasia relatives in some studies.
4,5
However, to the best of our knowl-
edge, the ATM Ser49Cys and ATM Ser707Pro missense mutations do
not cause ataxia telangiectasia in homozygotes,
19
so are likely not as
detrimental to the function of the ATM protein as those truncating
and missense ATM mutations that cause ataxia telangiectasia in the
homozygous state. Thus, although truncating and missense mutations
severe enough to cause ataxia telangiectasia might elevate the risk of
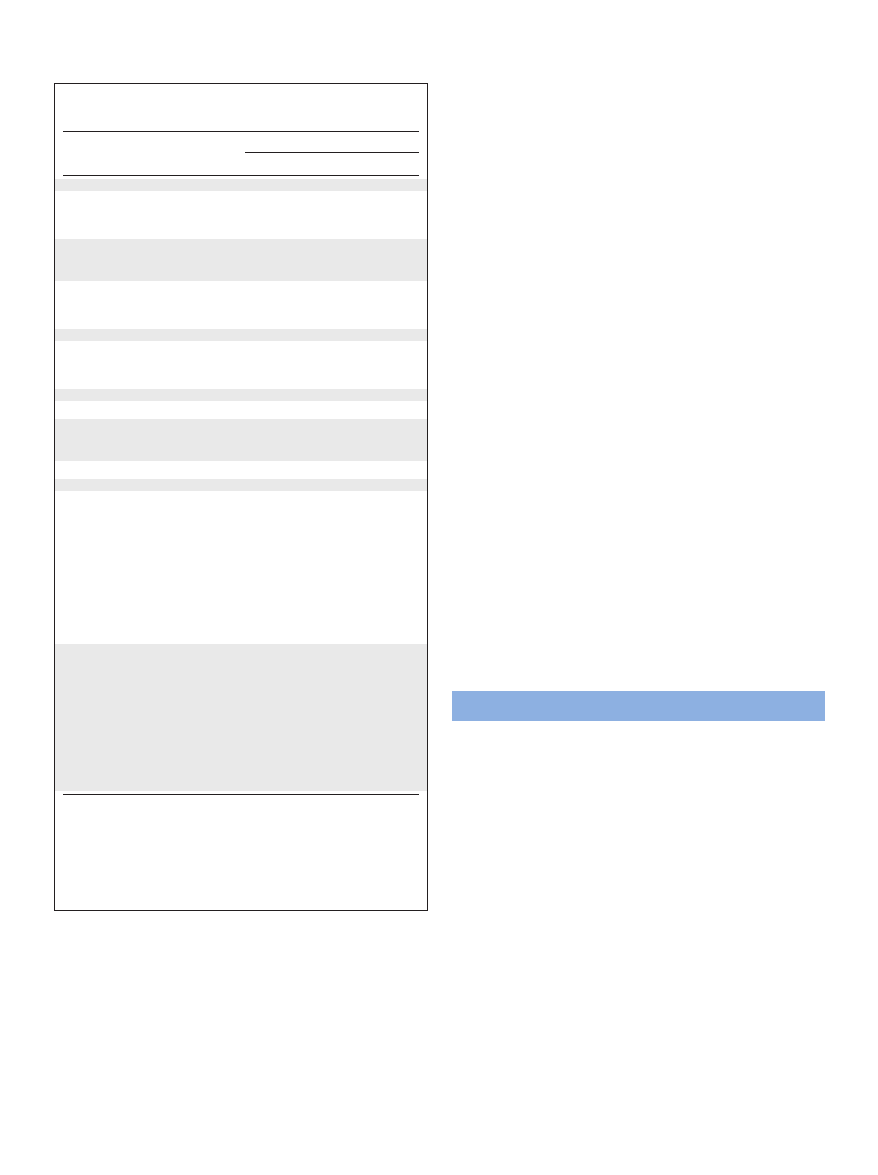
Table 1. Baseline Characteristics of Participants From the General
Population With and Without Cancer Developed
During 36 Years of Follow-Up
Characteristic
Disease Status
With Cancer
Without Event
No. of participants
2,056
8,261
Female sex
No.
1,120
4,559
%
55
55
Age, years
Median
52
ⴱ
43
Range
45-58
34-52
Body mass index, kg/m
2
Median
25
ⴱ
24
Range
22-27
22-27
Smoking, %
64
ⴱ
54
Alcohol consumption, g/wk
Median
0
ⴱ
0
Range
0-84
0-108
Women using OCD, %†
5
ⴱ
14
Nulliparous (women only), %
22
ⴱ
33
Parity (women only), No.
Median
2
ⴱ
1
Range
1-2
0-2
Postmenopausal women, %
56
ⴱ
33
Women using HRT, %‡
23
ⴱ
13
ATM Ser49Cys status
Noncarriers
No.
1,995
8,065
%
97.0
97.6
Heterozygotes
No.
60
195
%
2.9
2.4
Homozygotes
No.
1
1
%
0.05
0.01
ATM Ser707Pro status
Noncarriers
No.
2,012
8.086
%
97.9
97.9
Heterozygotes
No.
44
174
%
2.1
2.1
Homozygotes
No.
0
1
%
0
0.01
NOTE. Values were at study entry and were calculated on a slightly varying
number of individuals, depending on availability of data. Level of significance
was calculated by using the Mann-Whitney U Test or the Pearson
2
test.
Abbreviations: OCD, oral contraceptive drugs; HRT, hormone replace-
ment therapy.
ⴱ
P
⬍ .001.
†Use of oral contraceptive drugs at study entry.
‡Use of hormonal replacement therapy at study entry.
Risk of Cancer by ATM Missense Mutations in General Population
www.jco.org
© 2008 by American Society of Clinical Oncology
3059
cancer substantially in the heterozygous state, it is likely that less
detrimental missense mutations found relatively often in the general
population, such as ATM Ser49Cys and ATM Ser707Pro, do not in-
crease the risk of cancer to the same extent. Furthermore, it is also
possible that the increased cancer risk of relatives of patients with
ataxia telangiectasia is polygenic and stems from a cluster of unknown
common mutations that are segregated in ataxia telangiectasia fami-
lies, unlike in individuals from the general population, such as those
included in our study.
We could not confirm the two- to five-fold risk of breast cancer
associated with ATM Ser49Cys or ATM Ser707Pro heterozygosity ob-
served by others.
8-10
Studies that originally demonstrated an increased
risk of breast cancer in ATM Ser49Cys heterozygotes were small,
8,9
and
a recent report by the Breast Cancer Association Consortium also
failed to show an association between ATM Ser49Cys heterozygosity
and an increased risk of breast cancer.
11
Likewise, the study that
originally demonstrated an association between ATM Ser707Pro het-
erozygosity and an increased risk of breast cancer was a case-control
study with a much smaller study population than ours.
10
Our results
are also in accordance with a study by Spurdle et al
12
that showed ATM
Ser707Pro heterozygosity to be unassociated with breast cancer risk.
Originally, an association between ATM mutations and breast cancer
was suspected, because relatives of patients with ataxia telangiectasia
had an increased risk of breast cancer.
4,5
However, a recent study by
Renwick et al
19
has shown that only ATM mutations that are known to
cause ataxia telangiectasia in the homozygous state predispose to
breast cancer in heterozygotes. This finding agrees with our result that
neither ATM Ser49Cys nor ATM Ser707Pro heterozygosity predispose
to breast cancer.
ATM Ser49Cys appears to predispose to several other cancer
subtypes. In accordance with this, other mutations in cell cycle regu-
latory genes (eg, CHEK2*1100delC
20
) are known to predispose to
certain cancer subtypes, although they do not increase the overall risk
of cancer. It is becoming increasingly clear that there is a high degree of
communication between ATM and ATM- and rad3-related kinase
(ATR) and that there is some overlap in DNA repair pathways con-
trolled by these two.
21
The contribution of ATR to these DNA repair
pathways may be greater in some tissues than others. An impairment
of ATM caused by ATM Ser49Cys might, therefore, have a greater
impact on some cell types than others, which would result in an
increased susceptibility to certain cancer subtypes without an overall
elevation of the risk of cancer. Our observed association of ATM
Ser49Cys heterozygosity with an increased risk of melanoma is biolog-
ically plausible, as recent studies have shown ATM to be important for
DNA repair in response to UV light.
22,23
Furthermore, even when we
correct this finding for 26 different comparisons by using the Bonfer-
roni method (P
⫽ .05 ⫼ 26 ⫽ .002), this finding remains highly
significant. This association is interesting, because relatively few
melanoma-predisposing genes have been discovered so far. Given that
2.5% of the Danish population are heterozygous for ATM Ser49Cys
and that we estimated a hazard ratio for melanoma of 4.8, the corre-
sponding population attributable fraction is 9%. This means that
the incidence of melanoma in Denmark would decrease by 9% if ATM
Ser49Cys was not present in the Danish population. However, our
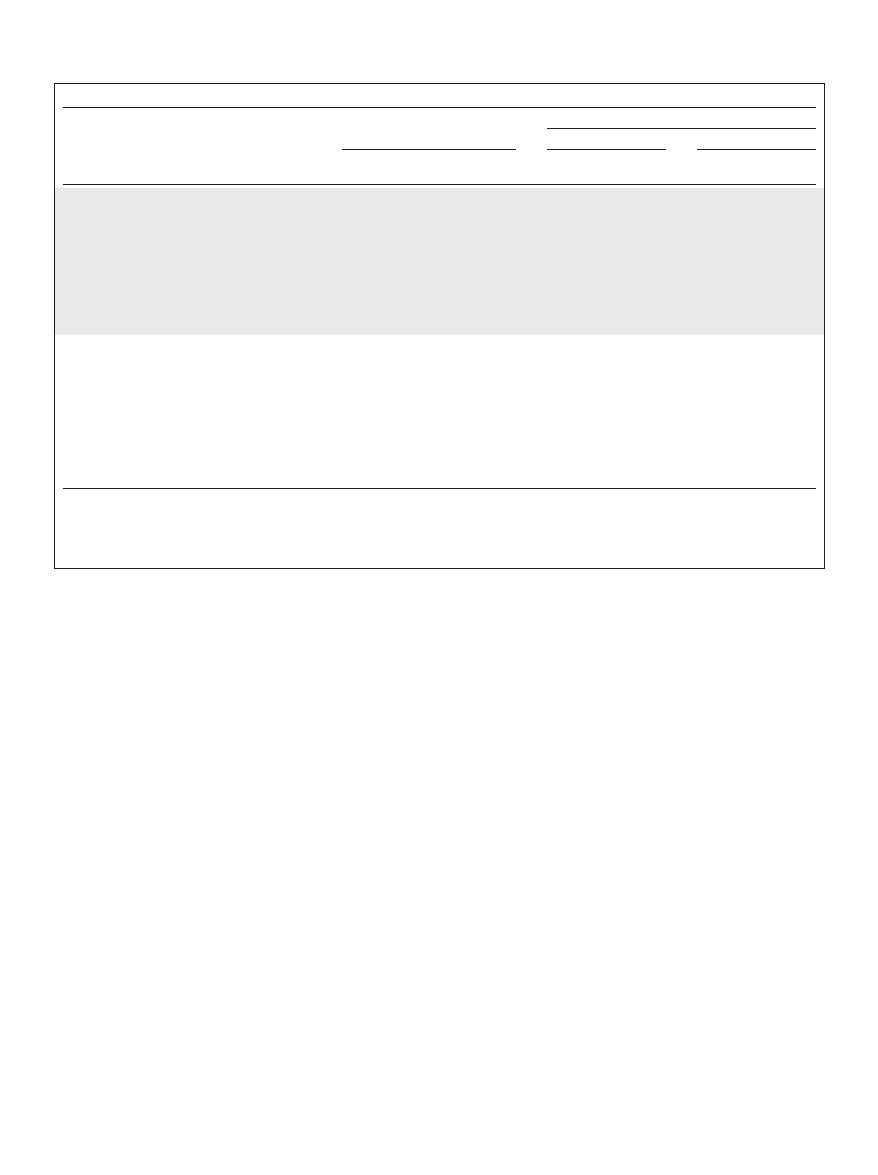
Table 2. Incidence and Risk of Any First Cancer According to Genotype in the General Population During 36 Years of Follow-Up
Genotype
No. of
Participants
No. of
Cancers
Incidence
Risk
Age
Multifactorial†
No.
ⴱ
95% CI
Log-Rank
P
Adjusted
HR
95% CI
Adjusted
HR
95% CI
ATM Ser49Cys
Overall
Noncarriers
10,059
1,995
67
64 to 70
1.0
1.0
Heterozygotes
255
60
79
61 to 102
.097
1.2
1.0 to 1.6
1.2
0.9 to 1.5
Women
Noncarriers
5,546
1,092
66
62 to 70
1.0
1.0
Heterozygotes
131
27
69
47 to 101
.61
1.1
0.8 to 1.6
1.0
0.7 to 1.5
Men
Noncarriers
4,513
903
67
63 to 72
1.0
1.0
Heterozygotes
124
33
89
64 to 126
.08
1.4
1.0 to 1.9
1.4
0.9 to 2.0
ATM Ser707Pro
Overall
Noncarriers
10,096
2,011
67
64 to 70
1.0
1.0
Heterozygotes
218
44
67
50 to 90
.57
0.9
0.7 to 1.2
0.8
0.6 to 1.2
Women
Noncarriers
5,554
1,094
66
62 to 70
1.0
1.0
Heterozygotes
123
25
67
45 to 99
.69
0.9
0.6 to 1.4
0.8
0.5 to 1.3
Men
Noncarriers
4,542
917
68
63 to 72
1.0
1.0
Heterozygotes
95
19
67
43 to 106
.67
0.9
0.6 to 1.4
0.8
0.5 to 1.3
NOTE. ATM Ser707Pro homozygotes were excluded in analysis of ATM Ser49Cys, and vice versa for analysis of ATM Ser707Pro.
Abbreviation: HR, hazard ratio.
ⴱ
Incidence reported per 10,000 person-years.
†Multifactorial adjustment for both sexes included age, sex, body mass index, weekly alcohol intake, smoking status and history, and the following in addition for
women: parity, nulliparity, use of oral contraceptive drugs, menopausal status, and use of hormonal replacement therapy.
Dombernowsky et al
3060
© 2008 by American Society of Clinical Oncology
J
OURNAL OF
C
LINICAL
O
NCOLOGY
findings were based on only seven heterozygotes with melanoma;
therefore, our estimated hazard ratio and population attributable frac-
tion could be overinflated by chance alone. In support of a role for
ATM Ser49Cys heterozygosity in prostate cancer, ATM P1054R het-
erozygosity also was associated with this disease.
6
This study also shows that ATM Ser49Cys is associated with
cancer of the oral cavity/pharynx and that ATM Ser707Pro is associ-
ated with thyroid/other endocrine tumors and cancer of corpus uteri.
At this point there is little or no additional evidence to support an
association with these cancer subtypes. Therefore, these findings ei-
ther could be accidental findings, caused in part to the low incidence of
cancer of the oral cavity/pharynx, thyroid/other endocrine tumors,
and cancer of corpus uteri in our study, or could represent real asso-
ciations observed for the first time.
There are some limitations to our study. First, as we performed
multiple comparisons, some of our findings could represent chance
findings rather than real phenomena. In exploratory analyses, we
tested two ATM mutations for the risk of 26 different cancer subtypes
and would therefore expect two to three associations to be significant
because of chance alone. However, we detected three significant asso-
ciations for ATM Ser49Cys heterozygosity and two significant associ-
ations for ATM Ser707Pro heterozygosity, so two to three of these
associations could represent real phenomena. We also found that
ATM Ser707Pro heterozygosity was associated with an increased risk
of other cancers, but we did not report this, because we believe this is a
highly unlikely finding. Second, both ATM Ser49Cys and ATM
Ser707Pro heterozygosity are relatively rare, so increased or decreased
risk is hard to detect, particularly for rare cancer subtypes, which
suggests that we easily could have overlooked other associations.
Third, our knowledge of some cancer risk factors was limited. Most
important, our knowledge of melanoma risk factors was incomplete.
Although we did adjust for the most relevant cancer risk factors, we
cannot completely exclude the possibility of confounding by other risk
factors on some of the observed associations. Fourth, participants
were genotyped only if they attended the 1991 to 1994 or 2001 to 2003
examinations of the Copenhagen City Heart Study. A selection bias
may have occurred if death or morbidity prevented certain individuals
from attending these examinations. However, two observations make
substantial selection bias against genotype less likely: 1) age percentiles
for noncarriers and heterozygotes display a linear relationship, as
would be expected if no selection occurred against heterozygotes; and
2) both genotype distributions are in Hardy-Weinberg equilibrium.
Thus, we do not consider selection bias against heterozygosity likely.
Fifth, we investigated only two of numerous reported ATM missense
Table 3. Incidence and Risk of Cancer Subtypes According to Genotype in the General Population During 36 Years of Follow-Up
Genotype
No. of
Participants
No. of
Cancers
Incidence
Risk
No.
95% CI
Log-Rank P
ⴱ
Age
Multifactorial†
Crude
Bonferroni‡
Adjusted
HR
95% CI
Adjusted
HR
95% CI
ATM Ser49Cys
Breast cancer in women only
Noncarriers
5,546
286
17
15 to 19
1.0
1.0
Heterozygotes
131
7
17
8 to 36
.90
NA
1.0
0.5 to 2.2
0.8
0.3 to 2.0
Melanoma
Noncarriers
10,059
59
2
2 to 2
1.0
1.0
Heterozygotes
255
7
9
4 to 19
⬍ .001
⬍ .001
4.8
2.2 to 11
4.8
2.2 to 11
Prostate cancer in men only
Noncarriers
4,513
116
8
7 to 10
1.0
1.0
Heterozygotes
124
7
18
9 to 38
.04
.99
2.2
1.0 to 4.7
2.3
1.1 to 5.0
Cancer of the oral cavity/pharynx
Noncarriers
10,059
32
1
1 to 1
1.0
1.0
Heterozygotes
255
3
4
1 to 12
.02
.52
3.7
1.1 to 12
3.4
1.1 to 11
ATM Ser707Pro
Breast cancer in women only
Noncarriers
5,554
289
17
15 to 19
1.0
1.0
Heterozygotes
123
4
10
4 to 27
.24
NA
0.6
0.2 to 1.5
0.6
0.2 to 1.6
Thyroid/other endocrine tumors
Noncarriers
10,096
4
0
0 to 0
1.0
1.0
Heterozygotes
218
1
2
0 to 10
.01
.26
10
1.2 to 94
10
1.1 to 93
Cancer of the corpus uteri in women only
Noncarriers
5,553
75
4
3 to 5
1.0
1.0
Heterozygotes
123
5
13
5 to 31
.02
.52
2.7
1.1 to 6.7
2.7
1.0 to 7.6
NOTE. ATM Ser707Pro homozygotes were excluded in analysis of ATM Ser49Cys, and vice versa for analysis of ATM Ser707Pro. Numbers vary slightly because
of differences in availability of data.
Abbreviation: HR, hazard ratio.
ⴱ
Incidence reported per 10,000 person-years.
†Multifactorial adjustment for melanoma and thyroid/other endocrine tumors included age and sex; for breast cancer: age, body mass index, alcohol consumption,
use of oral contraceptive drugs, use of hormonal replacement therapy, menopausal status, parity, and nulliparity; for cancer of the oral cavity/pharynx: age, sex,
smoking, smoking history, and alcohol consumption; for cancer of corpus uteri: age, body mass index, parity, and menopausal status; and for prostate cancer: age
and body mass index.
‡Corrected for 26 different comparisons (26 different cancer subtypes) for each mutation by using the Bonferroni method (crude P value multiplied by 26).
Risk of Cancer by ATM Missense Mutations in General Population
www.jco.org
© 2008 by American Society of Clinical Oncology
3061
mutations. Therefore, we cannot exclude that other mutations in this
gene may influence the risk of cancer in the general population.
Finally, misclassification of cancer end points may have occurred. This
is not likely, however, because we had 100% follow-up on participants
and because complete records of hospital admissions and deaths exist.
Furthermore, the Danish National Cancer Registry identifies 98% of
all cancers in Denmark.
24
In conclusion, ATM missense mutations do not increase the risk
of cancer overall or of breast cancer in the general population; how-
ever, we observed in exploratory analyses that ATM missense muta-
tions may be associated with an increased risk of other cancer
subtypes. As we did multiple comparisons, some of these findings
could represent chance findings rather than real phenomena.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS
OF INTEREST
The authors indicated no potential conflicts of interest.
AUTHOR CONTRIBUTIONS
Conception and design: Sarah Louise Dombernowsky, Maren Weischer,
Kristine Højgaard Allin, Stig Egil Bojesen, Anne Tybjærg-Hansen,
Børge Nordestgaard
Financial support: Anne Tybjærg-Hansen, Børge Nordestgaard
Administrative support: Børge Nordestgaard
Provision of study materials or patients: Stig Egil Bojesen, Anne
Tybjærg-Hansen, Børge Nordestgaard
Collection and assembly of data: Sarah Louise Dombernowsky, Maren
Weischer, Kristine Højgaard Allin, Stig Egil Bojesen, Anne
Tybjærg-Hansen, Børge Nordestgaard
Data analysis and interpretation: Sarah Louise Dombernowsky, Maren
Weischer, Stig Egil Bojesen, Anne Tybjærg-Hansen, Børge Nordestgaard
Manuscript writing: Sarah Louise Dombernowsky, Maren Weischer,
Børge Nordestgaard
Final approval of manuscript: Sarah Louise Dombernowsky, Maren
Weischer, Kristine Højgaard Allin, Stig Egil Bojesen, Anne
Tybjærg-Hansen, Børge Nordestgaard
REFERENCES
1. Shiloh Y: The ATM-mediated DNA-damage
response: Taking shape. Trends Biochem Sci 31:
402-410, 2006
2. Khanna KK, Chenevix-Trench G: ATM and
genome maintenance: Defining its role in breast
cancer susceptibility. J Mammary Gland Biol Neo-
plasia 9:247-262, 2004
3. Gatti RA, Tward A, Concannon P: Cancer risk
in ATM heterozygotes: A model of phenotypic and
mechanistic differences between missense and
truncating mutations. Mol Genet Metab 68:419-423,
1999
4. Swift M, Morrell D, Massey RB, et al: Inci-
dence of cancer in 161 families affected by ataxia-
telangiectasia. N Engl J Med 325:1831-1836, 1991
5. Thompson D, Duedal S, Kirner JFR, et al:
Cancer risks and mortality in heterozygous ATM
mutation carriers. J Natl Cancer Inst 97:813-822,
2005
6. Ange`le S, Falconer A, Edwards SM, et al:
ATM polymorphisms as risk factors for prostate
cancer development. Br J Cancer 91:783-787, 2004
7. Kim JH, Kim H, Lee KY, et al: Genetic poly-
morphisms of ataxia telangiectasia mutated affect
lung cancer risk. Hum Mol Genet 15:1181-1186,
2006
8. Stredrick DL, Garcia-Closas M, Pineda MA,
et al: The ATM missense mutation p.Ser49Cys
(c. 146C
⬎ G) and the risk of breast cancer. Hum
Mutat 27:538-544, 2006
9. Buchholz TA, Weil MM, Ashorn CL, et al:
A Ser49Cys variant in the ataxia telangiectasia, mu-
tated, gene that is more common in patients with
breast carcinoma compared with population con-
trols. Cancer 100:1345-1351, 2004
10. Do¨rk T, Bendix R, Bremer M, et al: Spectrum
of ATM gene mutations in a hospital-based series of
unselected breast cancer patients. Cancer Res 61:
7608-7615, 2001
11. Cox A, Dunning AM, Garcia-Closas M, et al:
A common coding variant in CASP8 is associated
with breast cancer risk. Nat Genet 39:352-358, 2007
12. Spurdle AB, Hopper JL, Chen X, et al: No
evidence for association of ataxia-telangiectasia mu-
tated gene T2119C and C3161G amino acid substi-
tution variants with risk of breast cancer. Breast
Cancer Res 4:R15, 2002
13. Khanna KK, Keating KE, Kozlov S, et al: ATM
associates with and phosphorylates p53: Mapping
the region of interaction. Nat Genet 20:398-400,
1998
14. Young DB, Jonnalagadda J, Gatei M, et al:
Identification of domains of ataxia-telangiectasia
mutated required for nuclear localization and chro-
matin association. J Biol Chem 280:27587-27594,
2005
15. Bojesen SE, Tybjærg-Hansen A, Nordestgaard
BG: Integrin beta3 Leu33Pro homozygosity and risk
of cancer. J Natl Cancer Inst 95:1150-1157, 2003
16. Storm HH: The Danish Cancer Registry, a
self-reporting national cancer registration system
with elements of active data collection. IARC Sci
Publ:220-236, 1991
17. Storm HH, Michelsen EV, Clemmensen IH, et
al: The Danish Cancer Registry: History, content,
quality and use. Dan Med Bull 44:535-539, 1997
18. Khoury MJ, Beaty TH, Cohen BH: Fundamen-
tals of Genetic Epidemiology. New York, NY, Oxford
University Press, 1993
19. Renwick A, Thompson D, Seal S, et al: ATM
mutations that cause ataxia-telangiectasia are breast
cancer susceptibility alleles. Nat Genet 38:873-875,
2006
20. Weischer M, Bojesen SE, Tybjærg-Hansen A,
et al: Increased risk of breast cancer associated with
CHEK2*1100delC. J Clin Oncol 25:57-63, 2007
21. Hurley PJ, Bunz F: ATM and ATR: Compo-
nents of an integrated circuit. Cell Cycle 6:414-417,
2007
22. Hannan MA, Hellani A, Al-Khodairy FM, et al:
Deficiency in the repair of UV-induced DNA damage
in human skin fibroblasts compromised for the ATM
gene. Carcinogenesis 23:1617-1624, 2002
23. Oakley GG, Loberg LI, Yao JQ, et al: UV-
induced hyperphosphorylation of replication protein
a depends on DNA replication and expression of
ATM protein. Mol Biol Cell 12:1199-1213, 2001
24. Storm HH: Completeness of cancer registra-
tion in Denmark 1943-1966 and efficacy of record
linkage procedures. Int J Epidemiol 17:44-49, 1988
■ ■ ■
Dombernowsky et al
3062
© 2008 by American Society of Clinical Oncology
J
OURNAL OF
C
LINICAL
O
NCOLOGY
Wyszukiwarka
Podobne podstrony:
Functional and Computational Assessment of Missense Variants in the Ataxia Telangiectasia Mutated (A
Spectrum of ATM Gene Mutations in a Hospital based Series of Unselected Breast Cancer Patients
Fake crop of Baptistic malicious spirits dummy baptism in the Spirit as taught by pastor John Torell
Risky feelings Why a 6 percent risk of cancer does not always feel like 6 percent
Functional improvements desired by patients before and in the first year after total hip arthroplast
Mutations in the CgPDR1 and CgERG11 genes in azole resistant C glabrata
[13]Role of oxidative stress and protein oxidation in the aging process
Functional improvements desired by patients before and in the first year after total hip arthroplast
Unsolved Mysteries An Exhibition of Unsolved Mysteries and Enigmatic Findings in the History of Hum
Nadelhoffer; On The Importance of Saying Only What You Believe in the Socratic Dialogues
Jażdżewska, Iwona The Warsaw – Lodz Duopolis in the light of the changes in the urban population de
J Leigh Globalization Reflections of Babylon Intercultural Communication and Globalization in the
Interaction of fraternal birth order and handedness in the
2000 Influence of Fiber Fermentability on Nutrient Digestion in the Dog
Alan L Mittleman A Short History of Jewish Ethics Conduct and Character in the Context of Covenant
Sources of Moral Obligation to Non Muslims in the Fiqh Al Aqalliyyat
DANN Changing patterns of violence at Qustul and Ballana in the post Meroitic period Part One The Hu
więcej podobnych podstron