The Journal of Nutrition
Proceedings of the Fourth International Scientific Symposium on Tea and Human Health
A Review of the Epidemiological Evidence on
Tea, Flavonoids, and Lung Cancer
1–3
Ilja C. W. Arts*
Department of Epidemiology, Nutrition, and Toxicology Research Institute Maastricht (NUTRIM), Maastricht University, 6200 MD,
Maastricht, The Netherlands
Abstract
Tea and its main bioactive ingredients, the flavonoids, have been associated with human cancer for several decades. In
this article, an overview is provided of observational epidemiological studies of lung cancer incidence in relation to intake of
green tea, black tea, flavonols/flavones, and catechins. A PubMed search was conducted in September 2007. Articles
were selected if they provided risk ratios (relative risk or odds ratio) for lung cancer and were of observational design
(cohort, case-control, or case-cohort). Three of 12 studies reported a significantly lower risk of lung cancer with a high
intake of flavonoids, whereas 1 study reported a significantly increased risk. After stratification by type of flavonoid,
catechin intake was no longer associated with lung cancer risk in 3 of 4 studies available. For tea, 4 of 20 studies reported
significantly reduced risks with high intake. Two studies found signficantly increased risk ratios, but both were older
studies. Findings were similar for green and black tea but became more significant when only methodologically sounder
cohort studies were considered. When tea intake and lung cancer were studied among never- or former smokers to
eliminate the confounding effect of smoking, 4 of 7 reported associations were significantly protective. In general, the
studies on tea, flavonoids, and lung cancer risk indicate a small beneficial association, particularly among never-smokers.
More well-designed cohort studies, in particular for catechins, are needed to strengthen the evidence on effects of long-
term exposure to physiological doses of dietary flavonoids.
J. Nutr. 138: 1561S–1566S, 2008.
Introduction
Tea consumption has been associated, both positively and
negatively, with human cancer for several decades. The first
epidemiological report on tea and cancer was published in 1966
(1). Since then, an increasing number of epidemiological studies
on tea intake and cancer have appeared. A PubMed search
conducted in September 2007 with the keywords ‘‘tea and
cancer and epidemiolog*’’ yielded 556 hits. In recent years the
collective evidence available for several types of cancer has been
summarized in systematic reviews and meta-analyses (2–4), but
to date, no such review has been published for lung cancer.
Tea, from a biological standpoint, is not a clearly defined
substance. All tea is produced from the leaves of Camellia
sinensis, but differences in processing result in several types of
tea, of which green and black tea are the most consumed world-
wide. Moreover, tea is a complex mixture of a large number of
bioactive components, including catechins, flavonols, lignans,
and phenolic acids. Theaflavins and thearubigins are present
only in black tea as a result of oxidative processes (5). All types
of tea and the major phenolic compounds present in tea have
been the subject of epidemiological studies. The debate is still
open as to which of these phenolic compounds might be of
primary importance, whether the combination of compounds is
essential, or if perhaps unknown components might be respon-
sible for any health-modulating effects of tea.
An earlier review on flavonoids and chronic diseases (6)
found evidence suggestive of a lower risk of lung cancer with a
higher intake of flavonols/flavones. However, at the time, only 4
cohort studies were available. Data from studies on asthma
incidence (7) and lung function (8) also suggested beneficial
effects from flavonoids. In an animal study, where rats were
given the major flavonol quercetin for 11 wk, the highest tissue
1
Published in a supplement to The Journal of Nutrition. Presented at the
conference ‘‘Fourth International Scientific Symposium on Tea and Human
Health,’’ held in Washington, DC at the U.S. Department of Agriculture on
September 18, 2007. The conference was organized by the Tea Council of the
U.S.A. and was cosponsored by the American Cancer Society, the American
College of Nutrition, the American Medical Women’s Association, the American
Society for Nutrition, and the Linus Pauling Institute. Its contents are solely the
responsibility of the authors and do not necessarily represent the official views of
the Tea Council of the U.S.A. or the cosponsoring organizations. Supplement
coordinators for the supplement publication were Lenore Arab, University of
California, Los Angeles, CA and Jeffrey Blumberg, Tufts University, Boston, MA.
Supplement coordinator disclosure: L. Arab and J. Blumberg received honorar-
ium and travel support from the Tea Council of the U.S.A. for cochairing the
Fourth International Scientific Symposium on Tea and Human Health and for
editorial services provided for this supplement publication; they also serve as
members of the Scientific Advisory Panel of the Tea Council of the U.S.A.
2
I. C. W. Arts is supported by a VENI Innovational Research Grant from the
Netherlands Organisation for Scientific Research—Earth and Life Sciences
(NWO-ALW).
3
Author disclosure: I. C. W. Arts received compensation from the supplement
sponsor for speaking at the Fourth International Scientific Symposium on Tea
and Human Health.
* To whom correspondence should be addressed. E-mail: ilja.arts@epid.
unimaas.nl.
0022-3166/08 $8.00
ª 2008 American Society for Nutrition.
1561S
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
concentrations were found in the lung (9). Taken together, these
data suggested a beneficial effect of tea and/or flavonoids on lung
health. This article provides an overview of observational ep-
idemiological studies considering lung cancer incidence or
mortality in relation to intake of green tea, black tea, flavonols/
flavones, and catechins.
Methods
A search in the PubMed database was conducted in September 2007
using the keywords tea, flavon*, flavan*, catechin, polyphenol, cancer,
tumor, cohort, case-control, case-cohort, intervention, meta-analysis,
and epidemiolog*. Reference lists of original articles on tea or flavonoids
and lung cancer and reviews on tea or flavonoids and cancer were
checked for relevant studies. Articles were selected for this review if they
provided risk ratios [relative risk or odds ratio (OR)] for lung cancer and
were of observational design (cohort, case-control, or case-cohort). Two
studies were excluded because no risk ratios were presented (10,11).
Studies on both incidence and mortality were included, but only 2
articles used lung cancer mortality data (12,13). From the articles, we
retrieved the number and gender of the participants, years of follow-up
(cohort and case-cohort studies only), and type of tea and/or flavonoids
studied. The most adjusted risk estimates, comparing the highest versus
the lowest intake category, corresponding 95% confidence intervals (CI),
and P-values for dose-response trend tests were extracted for this review.
If the original article did not present aggregated risk estimates, data for
subgroups (e.g., male/female, smokers/nonsmokers) were taken instead.
The 3 studies that did not specify the type of tea were from the United
States, Canada, and Sweden and were assumed to pertain to black tea.
Flavonols and flavones were grouped together because the intake of
flavones is minor compared with the intake of flavonols.
Case-control studies are vulnerable to recall bias, a phenomenon that
leads to attenuation of associations and that occurs because diseased
subjects may remember their diet differently from control subjects.
Therefore, results from cohort studies and case-control studies were also
discussed separately. A second major methodological issue in the analysis
of observational studies is confounding. Confounding is particularly
important when weak associations are studied in the presence of strong
confounders. In the case of the tea/flavonoid-lung cancer association,
smoking is one such strong confounder. Even after meticulous adjust-
ment for smoking behavior, residual confounding may exist. To reduce
the residual confounding presented by the strong smoking confounder,
we also summarized studies that only considered never- or former
smokers who had quit .20 y ago.
Results
Twelve studies, including 8 cohort studies, reported on the
association between intake of flavonoids and lung cancer
incidence (Table 1). None of the flavonoid studies considered
lung cancer mortality. All studies, except those by Arts et al.
(18,19) reported risk estimates for flavonols/flavones. More
recent studies have started to include catechins as well. Three
articles reported a significantly lower risk of lung cancer with a
high intake of flavonoids (15,17,20), whereas 1 article (24)
reported a significantly increased risk. The association between
flavonol/flavone intake and lung cancer incidence was similar to
that for flavonoids as a whole, but leaving out the methodolog-
ically less strong case-control studies allowed a stronger sug-
gestion of a protective association to emerge. Of the 6 cohort
studies, 3 showed a significant inverse association, and 3 showed
no effect. Only 1 of 4 studies on catechins and lung cancer found
a significant effect, with a risk ratio of 0.94 and a 95% CI of
0.91–0.98 (20). Leaving out the case-control study by Lagiou
et al. (24) did not change the findings for catechins.
On the association of tea and lung cancer, 20 studies were
published, including 6 cohort studies (Table 2). Two of the
cohort studies used data for cancer mortality instead of in-
cidence (12,13). Two studies were excluded from this overview
because they did not report a risk ratio estimate: Heilbrun et al.
(10), who were the first to report on tea and lung cancer in 1986,
found no significantly different age-adjusted lung cancer pro-
portion for frequent consumers of black tea. Huang et al. (11)
only mentioned that the association between green tea and
jasmine tea and lung cancer in their small case-control study was
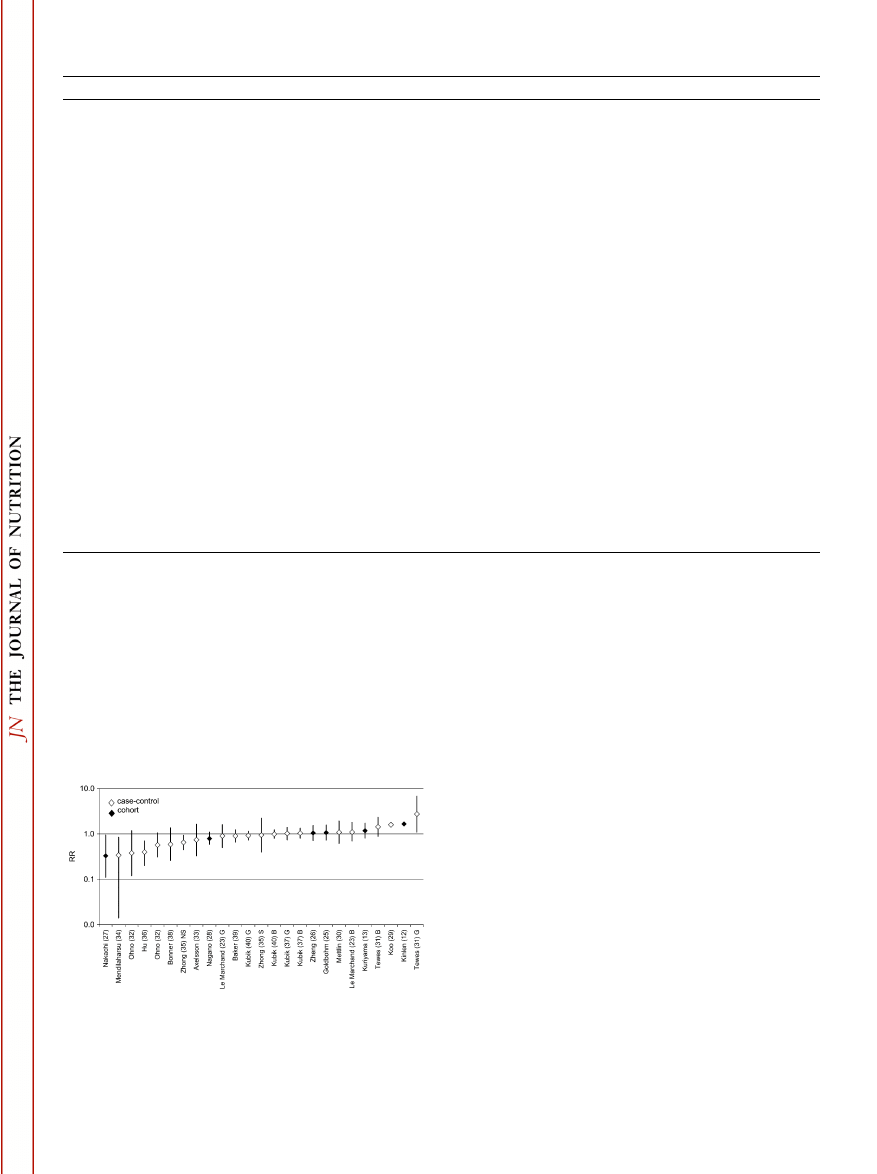
not significant. The overview of all studies on tea and lung
cancer is fairly symmetrical, although it appears slightly skewed
toward a protective association of tea intake (Fig. 1). Four risk
ratios reported were significantly below 1 (27,34–36). Two
studies reported risk ratios that were significantly higher than
1 (12,31). Both were older studies, and Kinlen et al. (12) did not
report a CI. Stratifying by type of tea consumed did not
substantially change the distribution of risk estimates (data
not shown). When the case-control studies were omitted from
consideration, few studies remained. Of the 3 cohort studies on
black tea, only the study by Kinlen et al. (12) showed a
significantly increased risk for lung cancer. For green tea, the
TABLE 1
Risk estimates from observational epidemiological studies on intake of flavonoids and risk of lung cancer
First author (ref)
Country
Year
Participants, n
Sex
Follow-up time, y
Type of flavonoids
RR
(95% CI)
1
P-trend
Prospective cohort studies
Hertog (14)
2
Netherlands
1994
740
M
5
Flavonols
1.02
(0.51 22.04)
0.96
Knekt (15)
Finland
1997
9,959
MF
24
Flavonols
0.53
(0.29 20.97)
—
Goldbohm (16)
Netherlands
1998
120,852
MF
4
Flavonols
0.99
(0.69 21.42)
0.68
Hirvonen (17)
Finland
2001
27,110
M
6
Flavonols
0.56
(0.45 20.69)
0.0001
Arts (18)
Netherlands
2001
728
M
10
Catechins
0.92
(0.41 22.07)
0.8
Knekt (7)
Finland
2002
5,218
M
30
Flavonols
0.64
(0.39 21.04)
0.02
Arts (19)
U.S.A.
2002
34,651
F
13
Catechins
0.94
(0.72 21.23)
0.94
Wright (20)
Finland
2004
27,111
M
11
Catechins 1 flavonols
0.94
(0.91 20.98)
0.005
Case-control studies
Garcia-Closas (21)
Spain
1998
103/206
3
F
Flavonols
0.98
(0.44 22.19)
0.98
De Stefani (22)
Uruguay
1999
541/540
M
Flavonols
0.80
(0.50 21.20)
—
Le Marchand (23)
U.S.A.
2000
582/582
MF
Flavonols
0.80
(0.50 21.40)
0.89
Lagiou (24)
Greece
2004
154/145
F
Catechins
1.02
(0.70 21.49)
0.91
Flavonols
1.83
(1.22 22.72)
0.003
1
RR: relative risk for prospective cohort studies; OR for case-control studies; 95% CI in parentheses.
2
Lung cancer and gastrointestinal tract cancer combined.
3
Number of cases/controls.
1562S
Supplement
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
study by Nakachi et al. (27) was the only 1 of 3 cohort studies
that found a significantly decreased risk for lung cancer.
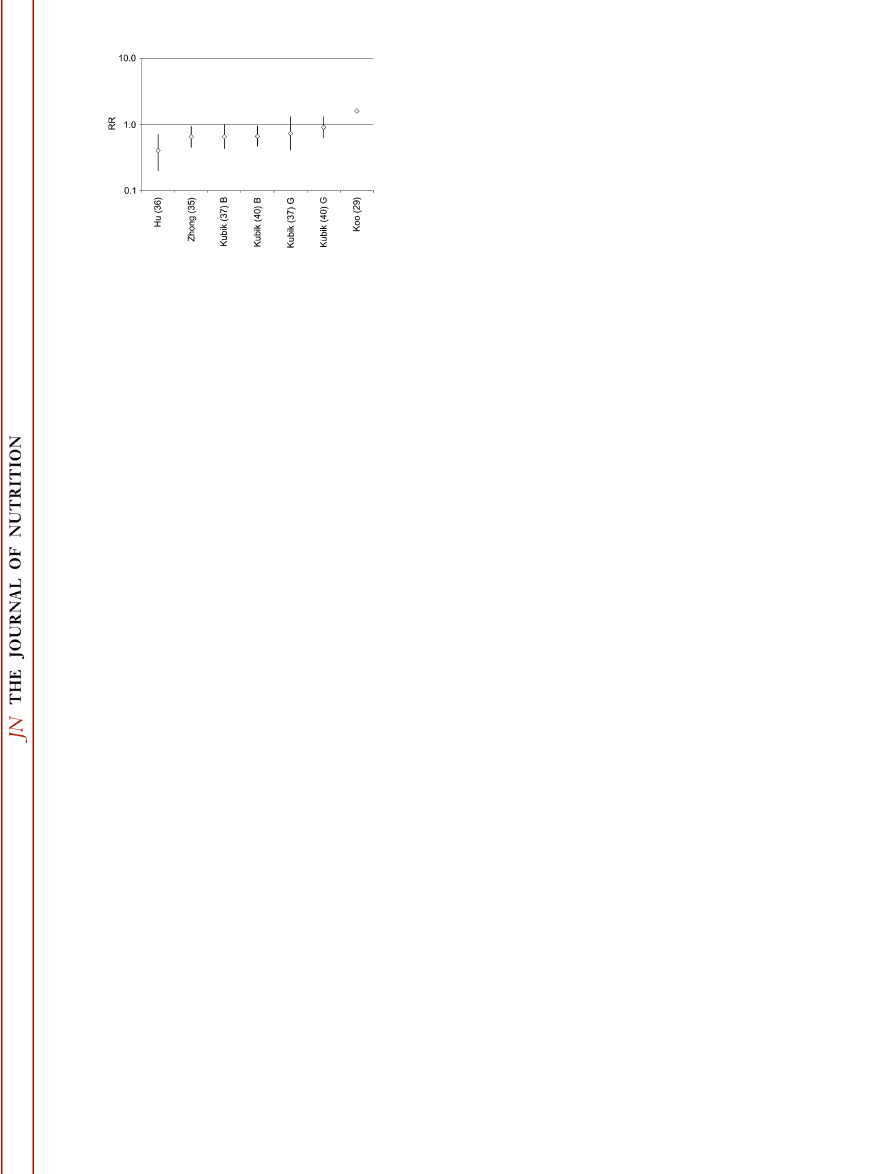
To study the association between tea intake and lung cancer
incidence without the confounding effect of smoking, studies
reporting risk estimates for never- or former smokers are summa-
rized in Figure 2. Four of seven studies that reported associations
among nonsmokers showed a significant protective association
for a high intake of tea. The other 3 associations were not
significantly different from 1. All studies were among women,
presumably because in most countries there are too few never-
smoking men to conduct meaningful analyses. In the studies by
Kubik et al. (37,40), nonsmokers were defined as women who
had never smoked and women who had quit .20 y ago. The
other 3 studies included never-smokers only. Only 2 studies on
flavonoid intake and lung cancer incidence presented risk
estimates for never-smokers. Garcia-Closas et al. (21) reported
that findings were similar to those for the whole sample (i.e., a
nonsignificant risk ratio of 0.98). Lagiou et al. (24) likewise
found no significant interaction between smoking status and
flavonoid intake, with risk estimates that were comparable to
those for the whole group.
Discussion
The collective evidence available so far from observational
epidemiological studies on tea, flavonoids, and lung cancer risk
tends toward a small beneficial association for green and black
tea, particularly among never-smokers, and for flavonols/
flavones but not for catechins. Studies that report increased
risks with a high intake of tea are mostly older studies that were
published at a time when tea was considered a possible car-
TABLE 2
Risk estimates from observational epidemiological studies on intake of tea and risk of lung cancer
First author (ref)
Country
Year
Participants, n
Sex
Follow-up time, y
Type of tea
RR
(95% CI)
1
P-trend
Prospective cohort studies
Kinlen (12)
2
UK
1988
14,085
M
17
Black
1.66
—
,0.05
Goldbohm (25)
Netherlands
1996
120,852
MF
4
Black
1.07
(0.73 21.57)
0.91
Zheng (26)
USA
1996
35,369
F
8
Nonherbal
1.05
(0.71 21.55)
0.54
Nakachi (27)
Japan
2000
8,552
MF
11
Green
0.33
(0.11 20.94)
—
Nagano (28)
Japan
2001
38,540
MF
13
Green
0.79
(0.59 21.10)
0.21
Kuriyama (13)
2
Japan
2006
40,530
MF
7
Green
1.18
(0.81 21.72)
0.36
Case-control studies
Koo (29)
China
1988
88/137
3
F
Any type
1.59
—
0.15
Mettlin (30)
USA
1989
569/569
MF
—
1.09
(0.62 21.93)
—
Tewes (31)
China
1990
200/200
F
Black
1.43
(0.88 22.33)
—
Green
2.74
(1.10 26.80)
—
Ohno (32)
Japan
1995
333/666
F
Green
0.38
(0.12 21.18)
0.03
M
0.57
(0.31 21.06)
0.05
Axelsson (33)
Sweden
1996
308/504
M
—
0.74
(0.33 21.64)
—
Mendilaharsu (34)
Uruguay
1998
427/428
M
Black
0.34
(0.01 20.84)
—
Le Marchand (23)
USA
2000
582/582
MF
Black
1.10
(0.70 21.80)
0.83
Green
0.90
(0.50 21.60)
0.62
Zhong (35)
China
2001
649/675
F
Green
0.65
(0.45 20.93)
4
—
0.94
(0.40 22.22)
5
—
Hu (36)
Canada
2002
161/483
F
—
0.40
(0.20 20.70)
0.001
Kubik (37)
Czech Republic
2004
451/1,710
F
Black
1.04
(0.80 21.34)
0.75
Green
1.02
(0.74 21.40)
0.94
Bonner (38)
China
2005
122/121
MF
Green
0.59
(0.26 21.37)
0.20
Baker (39)
USA
2005
993/986
MF
Black
0.90
(0.66 21.24)
0.93
Kubik (40)
Czech Republic
2007
569/2,120
F
Black
0.99
(0.80 21.23)
—
Green
0.92
(0.73 21.15)
—
1
Risk estimate for the highest versus the lowest category of intake: RR for prospective cohort studies; OR for case-control studies; 95% CI in parentheses.
2
Mortality.
3
Number of cases/controls.
4
Nonsmokers.
5
Smokers.
FIGURE 1
Risk estimates from observational epidemiological case-
control and cohort studies on intake of tea and risk of lung cancer.
Plotted are the most adjusted RR with 95% CI (if reported) for the
highest versus the lowest category of intake, sorted by increasing risk
ratio. F, females; M, males; NS, nonsmokers; G, green tea; S,
smokers; B, black tea.
Tea, flavonoids, and lung cancer
1563S
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
cinogenic and mutagenic (10,31). Several authors found that in
the Ames test, 1 cup of black or green tea was more mutagenic
than the smoke condensate of 1 cigarette (31,41). Epidemiolog-
ical data published later have not confirmed these concerns.
Peters et al. (42) found evidence for publication bias in a meta-
analysis on tea consumption and risk of stroke. We have not
examined publication bias. However, it seems unlikely that
studies finding increased lung cancer risks with increased tea or
flavonoid consumption would remain unpublished, given the
increased risk ratios reported in early studies and also in the light
of more recent reports regarding the increased mortality risks
that seem to be associated with taking antioxidant supplements,
particularly among smokers (43,44). Studies that found in-
creased risks with higher tea or flavonoid intake were mostly of
the case-control design. Only 1 cohort study found a risk
estimate that was significantly above 1: the 1988 study by Kinlen
et al. (12). In this study, tea intake was adjusted for smoking only
but not for other risk factors.
Accurate assessment of exposure to tea and/or flavonoids is
not easy. In general, food frequency questionnaires were not
designed to assess tea or flavonoid intake. In recent years,
assessment of tea consumption has received more attention (45),
but certainly baseline measurements of the older epidemiolog-
ical studies have yielded imprecise exposure estimates. Even if
the level of tea consumption is assessed accurately, differences in
cultivars and production methods and in brewing methods at
home also significantly influence the tea composition (46) and,
consequently, the internal exposure to bioactive ingredients.
Several databases have been used to estimate flavonoid intake
from dietary data. The Dutch values (46–49) that were most
frequently used in epidemiological studies are now part of the
comprehensive USDA flavonoid database (50), which has
rigorous quality control. It is my hope that more studies will
use this database in the near future. Inaccurate assessment of
exposure to tea/flavonoids has probably led to nondifferential
misclassification and an underestimation of the true associations
in the epidemiological studies presented here.
Although lung cancer is treated here as a single disease,
etiologically and histologically clearly distinct types of lung
cancer can be distinguished. Yet few authors of articles on this
subject have stratified their data by type of lung cancer. Le
Marchand et al. (23) found a stronger inverse trend with quer-
cetin intake among cases with squamous cell carcinoma (OR in
the highest quartile ¼ 0.5; 95% CI ¼ 0.2–1.9) compared with
cases with adenocarcinoma (OR ¼ 0.9; 95% CI ¼ 0.4–2.0).
Similarly, Zhong et al. (35) also reported a lower OR for
nonsmoking women with nonadenocarcinomas compared with
adenocarcinomas, but the numbers of cases were small, and
trends were not significant. Baker et al. (39), on the other hand,
found similar associations for black tea intake with different
subtypes (adeno-, squamous cell, small cell, and large cell
carcinoma) of lung cancer. More research is needed to determine
whether lung cancer type is of importance.
Residual confounding occurs if confounders, extraneous
factors that are associated with both the outcome and the
exposure under study, are not or insufficiently accounted for in
the statistical analysis. Studying associations in never-smokers is
an effective way of ruling out residual confounding by smoking.
Zhong et al. (35) have elegantly shown that the manner in which
models are adjusted for confounding by smoking can greatly
influence the results. The OR between green tea drinking and
lung cancer among women was 1.69 (95% CI ¼ 0.78–3.62)
without adjustment for smoking. When 4 categories of pack-
years were added to the model, the OR changed to 1.09, whereas
adding the number of cigarettes per day (as 3 categories) instead
gave an OR of 1.23. A smoothing technique, which allows more
precise adjustment for confounding, changed the estimated OR
to 1.23 and 0.94 for pack-years and number of cigarettes per
day, respectively. So, with use of different techniques to adjust
for smoking, the effect estimate changed significantly from 1.69
to 0.94, although none of the estimates was significant. In the
same article, Zhong and co-workers (35) also reported the OR
for never-smokers, which was 0.65 (95% CI ¼ 0.45–0.93) and
significant. Thus, residual confounding for strong confounders
such as smoking can lead to higher risk estimates in populations
where smoking is associated with tea drinking. Our overview of
studies among nonsmokers suggests that, indeed, protective
associations become more distinct in this group. On the other
hand, when tea drinking is associated with a healthy lifestyle,
associations may become more beneficial as a result of residual
confounding. More research among never-smokers is needed to
resolve this issue, taking into account exposure to environmental
smoke and other determinants of lung cancer among never
smokers.
In tea-drinking populations, the correlation between tea
intake and flavonoid intake is high. For example, in the Zutphen
Elderly Study in The Netherlands, the correlation between
catechins and tea was 0.98, making the 2 variables essentially
interchangeable (18). Which approach is preferred then, the
food-based one or the component-based approach? Of course
that depends on the hypothesized mechanism: if flavonoids are
considered to be the active compounds in tea, then it makes
more sense to look at flavonoids directly. In countries where tea
intake is low, such as many Mediterranean countries, other
sources of flavonoids will become important. However, if other
compounds in tea, or combinations of compounds, are believed
to be important, then tea would be the preferred exposure. In
that case, calculating flavonoid intake will merely introduce
additional error. The results presented in this overview show that
a similar picture emerges, whether tea or flavonoids are used as
exposure estimates. For catechins, too few studies have been
published to draw any conclusions. Despite its drawbacks,
observational epidemiology is the only type of research that is
able to assess the effects of long-term exposure to physiological
doses of bioactive compounds on real disease endpoints. It
therefore has great value in the study of the association between
intake of tea and flavonoids and lung cancer risk. Accumulating
more data from well-designed studies, together with more
FIGURE 2
Risk estimates from observational epidemiological case-
control studies on intake of tea and risk of lung cancer among never-
or former ($20 y ago) smokers. Plotted are the most adjusted RR with
95% CI (if reported) for the highest versus the lowest category of
intake, sorted by increasing RR. G, green tea; B, black tea.
1564S
Supplement
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
mechanistic intervention studies, will bring us closer to firm
conclusions about the health effects of tea and its bioactive
ingredients.
Other articles in this supplement include references (51–60).
Literature Cited
1.
Higginson J. Etiological factors in gastrointestinal cancer in man. J Natl
Cancer Inst. 1966;37:527–45.
2.
Sun CL, Yuan JM, Koh WP, Yu MC. Green tea, black tea and colorectal
cancer risk: a meta-analysis of epidemiologic studies. Carcinogenesis.
2006;27:1301–9.
3.
Sun CL, Yuan JM, Koh WP, Yu MC. Green tea, black tea and breast
cancer risk: a meta-analysis of epidemiological studies. Carcinogenesis.
2006;27:1310–5.
4.
Steevens J, Schouten LJ, Verhage BA, Goldbohm RA, van den Brandt
PA. Tea and coffee drinking and ovarian cancer risk: results from the
Netherlands Cohort Study and a meta-analysis. Br J Cancer. 2007;
97:1291–4.
5.
Balentine DA, Wiseman SA, Bouwens LCM. The chemistry of tea
flavonoids. Crit Rev Food Sci Nutr. 1997;37:693–704.
6.
Arts ICW, Hollman PCH. Polyphenols and disease risk in epidemiologic
studies. Am J Clin Nutr. 2005;81:317S–25S.
7.
Knekt P, Kumpulainen J, Jarvinen R, Rissanen H, Heliovaara M,
Reunanen A, Hakulinen T, Aromaa A. Flavonoid intake and risk of
chronic diseases. Am J Clin Nutr. 2002;76:560–8.
8.
Tabak C, Arts ICW, Smit HA, Heederik D, Kromhout D. Chronic
obstructive pulmonary disease and intake of catechins, flavonols, and
flavones. The MORGEN Study. Am J Respir Crit Care Med. 2001;
164:61–4.
9.
de Boer VCJ, Dihal AA, van der Woude H, Arts ICW, Wolffram S, Alink
GM, Rietjens IMCM, Keijer J, Hollman PCH. Tissue distribution of
quercetin in rats and pigs. J Nutr. 2005;135:1718–25.
10. Heilbrun LK, Nomura A, Stemmermann GN. Black tea consumption
and cancer risk: a prospective study. Br J Cancer. 1986;54:677–83.
11. Huang C, Zhang X, Qiao Z, Guan L, Peng S, Liu J, Xie R, Zheng L. A
case-control study of dietary factors in patients with lung cancer.
Biomed Environ Sci. 1992;5:257–65.
12. Kinlen LJ, Willows AN, Goldblatt P, Yudkin J. Tea consumption and
cancer. Br J Cancer. 1988;58:397–401.
13. Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y,
Tsubono Y, Tsuji I. Green tea consumption and mortality due to
cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study.
JAMA. 2006;296:1255–65.
14. Hertog MG, Feskens EJ, Hollman PC, Katan MB, Kromhout D. Dietary
flavonoids and cancer risk in the Zutphen Elderly Study. Nutr Cancer.
1994;22:175–84.
15. Knekt P, Jarvinen R, Seppanen R, Hellovaara M, Teppo L, Pukkala E,
Aromaa A. Dietary flavonoids and the risk of lung cancer and other
malignant neoplasms. Am J Epidemiol. 1997;146:223–30.
16. Goldbohm RA, Hertog MGL, Brants HAM, Van Poppel G, Van den
Brandt PA. Intake of flavonoids and cancer risk: a prospective cohort
study. In: Amado` R, Andersson H, Bardosz S, Serra F, editors.
Polyphenols in Food. Office for Official Publications of the European
Communities, Luxembourg 1998: Proceeding of the 1st workshop of
the COST 916 Action; 1997 Apr 16–9, Aberdeen, Scotland. EUR 18169
EN. p. 159–66.
17. Hirvonen T, Virtamo J, Korhonen P, Albanes D, Pietinen P. Flavonol and
flavone intake and the risk of cancer in male smokers (Finland). Cancer
Causes Control. 2001;12:789–96.
18. Arts ICW, Hollman PCH, Bueno de Mesquita HB, Feskens EJM,
Kromhout D. Dietary catechins and epithelial cancer incidence: The
Zutphen elderly study. Int J Cancer. 2001;92:298–302.
19. Arts ICW, Jacobs DR, Jr., Gross M, Harnack LJ, Folsom AR. Dietary
catechins and cancer incidence among postmenopausal women: the
Iowa Women’s Health Study (United States). Cancer Causes Control.
2002;13:373–82.
20. Wright ME, Mayne ST, Stolzenberg-Solomon RZ, Li Z, Pietinen P,
Taylor PR, Virtamo J, Albanes D. Development of a comprehensive
dietary antioxidant index and application to lung cancer risk in a cohort
of male smokers. Am J Epidemiol. 2004;160:68–76.
21. Garcia-Closas R, Agudo A, Gonzalez CA, Riboli E. Intake of specific
carotenoids and flavonoids and the risk of lung cancer in women in
Barcelona, Spain. Nutr Cancer. 1998;32:154–8.
22. De Stefani E, Boffetta P, Deneo-Pellegrini H, Mendilaharsu M, Carzoglio
JC, Ronco A, Olivera L. Dietary antioxidants and lung cancer risk: a
case-control study in Uruguay. Nutr Cancer. 1999;34:100–10.
23. Le Marchand L, Murphy SP, Hankin JH, Wilkens LR, Kolonel LN. Intake
of flavonoids and lung cancer. J Natl Cancer Inst. 2000;92:154–60.
24. Lagiou P, Samoli E, Lagiou A, Katsouyanni K, Peterson J, Dwyer J,
Trichopoulos D. Flavonoid intake in relation to lung cancer risk: case-
control study among women in Greece. Nutr Cancer. 2004;49:139–43.
25. Goldbohm RA, Hertog MG, Brants HA, van Poppel G, van den Brandt
PA. Consumption of black tea and cancer risk: a prospective cohort
study. J Natl Cancer Inst. 1996;88:93–100.
26. Zheng W, Doyle TJ, Kushi LH, Sellers TA, Hong CP, Folsom AR. Tea
consumption and cancer incidence in a prospective cohort study of
postmenopausal women. Am J Epidemiol. 1996;144:175–82.
27. Nakachi K, Matsuyama S, Miyake S, Suganuma M, Imai K. Preventive
effects of drinking green tea on cancer and cardiovascular disease:
epidemiological evidence for multiple targeting prevention. Biofactors.
2000;13:49–54.
28. Nagano J, Kono S, Preston DL, Mabuchi K. A prospective study of
green tea consumption and cancer incidence, Hiroshima and Nagasaki
(Japan). Cancer Causes Control. 2001;12:501–8.
29. Koo LC. Dietary habits and lung cancer risk among Chinese females in
Hong Kong who never smoked. Nutr Cancer. 1988;11:155–72.
30. Mettlin C. Milk drinking, other beverage habits, and lung cancer risk.
Int J Cancer. 1989;43:608–12.
31. Tewes FJ, Koo LC, Meisgen TJ, Rylander R. Lung cancer risk and
mutagenicity of tea. Environ Res. 1990;52:23–33.
32. Ohno Y, Wakai K, Genka K, Ohmine K, Kawamura T, Tamakoshi A,
Aoki R, Senda M, Hayashi Y, et al. Tea consumption and lung cancer
risk: a case-control study in Okinawa, Japan. Jpn J Cancer Res.
1995;86:1027–34.
33. Axelsson G, Liljeqvist T, Andersson L, Bergman B, Rylander R. Dietary
factors and lung cancer among men in west Sweden. Int J Epidemiol.
1996;25:32–9.
34. Mendilaharsu M, De Stefani E, Deneo-Pellegrini H, Carzoglio JC,
Ronco A. Consumption of tea and coffee and the risk of lung cancer in
cigarette-smoking men: a case-control study in Uruguay. Lung Cancer.
1998;19:101–7.
35. Zhong L, Goldberg MS, Gao YT, Hanley JA, Parent ME, Jin F. A
population-based case-control study of lung cancer and green tea
consumption among women living in Shanghai, China. Epidemiology.
2001;12:695–700.
36. Hu J, Mao Y, Dryer D, White K. Risk factors for lung cancer among
Canadian women who have never smoked. Cancer Detect Prev. 2002;
26:129–38.
37. Kubik AK, Zatloukal P, Tomasek L, Pauk N, Havel L, Krepela E,
Petruzelka L. Dietary habits and lung cancer risk among non-smoking
women. Eur J Cancer Prev. 2004;13:471–80.
38. Bonner MR, Rothman N, Mumford JL, He X, Shen M, Welch R, Yeager
M, Chanock S, Caporaso N, Lan Q. Green tea consumption, genetic
susceptibility, PAH-rich smoky coal, and the risk of lung cancer. Mutat
Res. 2005;582:53–60.
39. Baker JA, McCann SE, Reid ME, Nowell S, Beehler GP, Moysich KB.
Associations between black tea and coffee consumption and risk of lung
cancer among current and former smokers. Nutr Cancer. 2005;52:
15–21.
40. Kubik A, Zatloukal P, Tomasek L, Pauk N, Havel L, Dolezal J, Plesko I.
Interactions between smoking and other exposures associated with lung
cancer risk in women: diet and physical activity. Neoplasma. 2007;54:
83–8.
41. Nagao M, Takahashi Y, Yamanaka H, Sugimura T. Mutagens in coffee
and tea. Mutat Res. 1979;68:101–6.
42. Peters U, Poole C, Arab L. Does tea affect cardiovascular disease? A
meta-analysis. Am J Epidemiol. 2001;154:495–503.
43. Albanes D, Heinonen OP, Taylor PR, Virtamo J, Edwards BK, Rautalahti
M, Hartman AM, Palmgren J, Freedman LS, et al. Alpha-Tocopherol
and beta-carotene supplements and lung cancer incidence in the alpha-
tocopherol, beta-carotene cancer prevention study: effects of base-
line characteristics and study compliance. J Natl Cancer Inst. 1996;
88:1560–70.
Tea, flavonoids, and lung cancer
1565S
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
44. Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C.
Mortality in randomized trials of antioxidant supplements for primary
and secondary prevention: systematic review and meta-analysis. JAMA.
2007;297:842–57.
45. Hakim IA, Hartz V, Harris RB, Balentine D, Weisgerber UM, Graver E,
Whitacre R, Alberts D. Reproducibility and relative validity of a
questionnaire to assess intake of black tea polyphenols in epidemiolog-
ical studies. Cancer Epidemiol Biomarkers Prev. 2001;10:667–78.
46. Arts ICW, van de Putte B, Hollman PCH. Catechin contents of foods
commonly consumed in The Netherlands. 2. Tea, wine, fruit juices, and
chocolate milk. J Agric Food Chem. 2000;48:1752–7.
47. Hertog MGL, Hollman PCH, Van de Putte B. Content of potentially
anticarcinogenic flavonoids of tea infusions, wines, and fruit juices.
J Agric Food Chem. 1993;41:1242–6.
48. Hertog MGL, Hollman PCH, Katan MB. Content of potentially
anticarcinogenic flavonoids of 28 vegetables and 9 fruits commonly
consumed in the Netherlands. J Agric Food Chem. 1992;40:2379–83.
49. Arts ICW, van de Putte B, Hollman PCH. Catechin contents of foods
commonly consumed in The Netherlands. 1. Fruits, vegetables, staple
foods, and processed foods. J Agric Food Chem. 2000;48:1746–51.
50. USDA Database for the Flavonoid Content of Selected Foods. 2007.
Release 2.1 [database on the Internet]. Beltsville, MD: U.S. Department
of Agriculture. Available from: http://www.ars.usda.gov/Services/docs.
htm?docid¼6231.
51. Arab L, Blumberg JB. Introduction to the Proceedings of the Fourth
International Scientific Symposium on Tea and Human Health. J Nutr.
2008;138:1526S–8S.
52. Henning SM, Choo JJ, Heber D. Nongallated compared with gallated
flavan-3-ols in green and black tea are more bioavailable. J Nutr.
2008;138:1529S–34S.
53. Auger C, Mullen W, Hara Y, Crozier A. Bioavailability of polyphenon E
flavan-3-ols in humans with an ileostomy. J Nutr. 2008;138:
1535S–42S.
54. Song WO, Chun OK. Tea is the major source of flavan-3-ol and flavonol
in the U.S. diet. J Nutr. 2008;138:1543S–7S.
55. Kuriyama S. The relation between green tea consumption and cardio-
vascular disease as evidenced by epidemiological studies. J Nutr.
2008;138:1548S–53S.
56. Grassi D, Aggio A, Onori L, Croce G, Tiberti S, Ferri C, Ferri L,
Desideri G. Tea, flavonoids, and NO-mediated vascular reactivity.
J Nutr. 2008;138:1554S–60S.
57. Hakim IA, Chow HHS, Harris RB. Green tea consumption is associated
with decreased DNA damage among GSTM1 positive smokers regard-
less of their hOGG1 genotype. J Nutr. 2008;138:1567S–71S.
58. Kelly SP, Gomez-Ramirez M, Montesi JL, Foxe JJ. L-Theanine and
caffeine in combination affect human cognition as evidenced by oscil-
latory alpha-band activity and attention task performance. J Nutr.
2008;138:1572S–7S.
59. Mandel SA, Amit T, Kalfon L, Reznichenko L, Youdim MBH. Targeting
multiple neurodegenerative diseases etiologies with multimodal-acting
green tea catechins. J Nutr. 2008;138:1578S–83S.
60. Stote KS, Baer DJ. Tea consumption may improve biomarkers of insu-
lin sensitivity and risk factors for diabetes. J Nutr. 2008;138:
1584S–8S.
1566S
Supplement
at UNIWERSYTET PRZYRODNICZY WE WROCLAWIU on December 18, 2011
jn.nutrition.org
Downloaded from
Wyszukiwarka
Podobne podstrony:
A Review of The Outsiders Club Screened on?C 2 in October
The Epidemiology and Phenomenology of NSSI Behaviour Among Adolescents A Critical Review of the Lit
Book Review of The Color Purple
Short review of the book entitled E for?stasy
Book Review of The Burning Man
24 Variability of the European climate on the basis of differentiation of indicators of continentali
John Ringo The Legacy of the Aldenata 7 Watch On The Rhine
Phylogeny of the enterobacteriaceae based on genes encoding elongation factor Tu
A Review of the Antimicrobial Activity of Chitosan
Review of The New Economic Sociology
THE VACCINATION POLICY AND THE CODE OF PRACTICE OF THE JOINT COMMITTEE ON VACCINATION AND IMMUNISATI
Art of the Ridiculous Sublime On David Lynch s Lost Highway Slavoj Zizek
McDougall G , Report of the Independent Expert on Minority Issues
brainwashing a synthesis of the russian textbook on psychopolitics
więcej podobnych podstron