DIAGNOSTYKA FUNKCJONALNA
W FIZJOTERAPII W
NEUROLOGII
Akademia Wychowania Fizycznego w
Katowicach
prof.
dr hab. Józef
Opara
specjalista neurologii i
rehabilitacji
Nowoczesna rehabilitacja
neurologiczna
Michael P. Barnes
Standards in neurological
rehabilitation, June 1997
European Journal of Neurology (1997), 4, 325-331
European Federation of Neurological
Societies
EFNS Task Force
Hunters Moor Rehabilitation Centre, Hunters Road,
Newcastle, UK
Nowoczesna
rehabilitacja
Epidemiology in UK
per 100000 population Incidence Prevalence
in 1993 per year Total Disabled
_____________________________________________________
PD 20 180 72
MS
4
100
50
Stroke 220 600 360
SCI
2
60
50
SAH
15
50
?
Nowoczesna
rehabilitacja
EFNS Scientific Panel on Neurorehabilitation Task Force
on standards in neurological rehabilitation, June 1996:
(1) A questionnaire circulated to each
European member country has indicated a
significant lack of adequate neurological
rehabilitation facilities across Europe. Very
few countries have any established network
of neurological rehabilitation centres. Few
countries have adequately trained
neurological rehabilitation physicians,
therapists or nurses. Such poor facilities
should be seen in the context of the large
numbers and increasing prevalence of
people with neurological disabilities.
Nowoczesna
rehabilitacja
EFNS Task Force standards
1996
(2) The Task Force has summarized the
significant benefits that can follow from the
establishment of a dedicated and cost
effective neurological rehabilitation service
including functional improvement, reduction of
unnecessary complications, better co-
ordination and use of limited resources,
improved opportunities for education, training
and research and a clear point of contact for
the disabled person.
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
(3) The Task Force recommends minimum
standards for the prevention of neurological
disability including access to health education,
genetic counselling and emergency recourses.
The Task Force also encourages governments to
invest in improved legislation for accident
prevention.
(4) The Task Force has outlined some minimum standards
for the staffing of a neurological rehabilitation service
including improved training both for neurologists and
rehabilitation physicians. Such training could include a
cross-national training programme both for physicians
and other health care staff.
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
(5) The Task Force supports a two-tier system of
neurological services. We believe that disabled
individuals should have access to a regional specialist
service as well as a local community service. The
regional specialist service would cater for people with
more complicated and severe disabilities, including
spinal injury and severe brain injury. The regional
centres would provide specialist expertise for
wheelchairs and special seating, orthotics, continence
and urological services, aids and equipment including
communication aids and environmental controls,
prosthetics and driving assessment. The Task Force
additionally endorses the development of local and
community based rehabilitation teams with clear links
to the regional centre.
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
(6) The Task Force recognizes the
limited amount of rehabilitation
research and encourages individuals,
universities and governments to
invest more in rehabilitation
research. Such investment should
produce benefits for disabled people
and their carers and in the long term
benefits for the national economy
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
(7) The Task Force reaIizes that
neurological rehabilitation is poorly
developed both in Europe and the
world as a whole. We firmly endorse
international co-operation in this field
and are happy to co-operate with any
international organization in order to
develop such links for clinical,
educational or research initiatives.
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
(8) The Task Force encourages individual
countries to produce a document
summarizing their own situation with
regard to these standards and to
produce a timetable for action to
improve their situation. The EFNS Task
Force would be pleased to assist in the
publication of such deliberations or to
act as a focus for international
education and research or for sharing
of examples of good practice.
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
Rehabilitation has been defined as
:
an active process by which those disabled
by injury or disease achieve a full recovery
or if a full recovery is not possible realise
their optimal physical, mental and social
potential and are integrated into their most
appropriate environment.
(World Health Organization, 1980)
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
Definicja r
ehabilitacji
:
aktywny (czynny) proces dzięki któremu
osoby niepełnosprawne z powodu urazu
lub choroby uzyskują pełny powrót do
zdrowia, lub jeżeli pełne wyzdrowienie nie
jest możliwe uzyskują optymalny potencjał
fizyczny, psychiczny i społeczny i zostają
zintegrowani
ze swoim przystosowanym środowiskiem.
(WHO, 1980)
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
There are significant benefits from a
dedicated
neurological rehabilitation service:
Functional benefit
Reduction of unnecessary complications
Co-ordination and use of resources
Reduction of crisis admission to hospital
Lessened handicap
Cost effective
Education and teaching
Research
Point of contact
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
Korzyści
płynące z rehabilitacji
neurologiocznej:
Poprawa funkcjonalna
Zredukowanie do minimum (zbędnych) powikłań
Rzadsze przyjęcia do szpitala z powodu pogorszeń
Zmniejszenie niepełnosprawności
Obniżenie kosztów leczenia
Nowoczesna
rehabilitacja
EFNS Task Force standards 1996
Staffing
The Task Force recommends that every person with a
neurological disability should have access to support and
advice from a physician expert in neurological
rehabilitation
Multidisciplinary team
trained in the management
of neurological disabilities:
physiotherapy
occupational therapy
access to speech and language therapy
access to clinical neuropsychology
rehabilitation nursing
occasional and intermittent access to other relevant
disciplines
Multidyscyplinarny
zespół
rehabilitacyjny
(team)
• lekarz
• magister
fizjoterapii
• fizjoterapeuta
lic.
• terapeuta
zajęciowy
• logopeda
• asystent
socjalny
• technik
ortopeda
•
psycholog
• pielęgniarka
NOWOCZESNA REHABILITACJA
NEUROREHABILITACJA
(NEUROREHABILITACJA)
– CO TO JEST
?
Nowoczesna
rehabilitacja
Nowoczesna
rehabilitacja
Report of Pan European Consensus Meeting
on Stroke Management (Helsingborg,
Sweden,
8-10 November 1995):
at the start of rehabilitation every patient should have
access to rehabilitation services without prior
selection,
have his/her disability needs assessed as soon as
possible by a properly trained health professionals,
take part in a goal planning meeting involving all
rehabilitation professionals and family.
Nowoczesna
rehabilitacja
Report of Pan European Consensus Meeting on Stroke
Management (Helsingborg, Sweden, 8-10 Nov. 1995)
cont.
Rehabilitation should be centred on patient`s own goals.
The rehabilitation requires the intervention of an
interdisciplinary team constisting of physicians, nurses,
physiotherapists, occupational therapists, speech
therapists, neuropsychologists and others.
Any technique used in the management of disability
should be specified, targeted, intensive and patient-
centred.
No recomendation can be made on specific techniques
which might be used.
Nowoczesna
rehabilitacja
Report of Pan European Consensus Meeting on
Stroke Management (Helsingborg, Sweden, 8-10
Nov. 1995) cont.
G o a l s:
7.
Do roku 2005 co najmniej 70% osób
spośród tych którzy przeżyli udar
uzyska samodzielność w
czynnościach codziennych (ADL)
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006
on European Stroke Strategies
Kjellstrom T., Norrving B., Schtchkute
A. Cerebrovasc. Dis. 2007; 23: 229-41
Rehabilitation after Stroke
Goal for 2015
The goal for rehabilitation after stroke
is that three months after the onset of
stroke, over 70% of the surviving
patients are independent in their
activities of daily living.
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006 on European Stroke
Strategies
Kjellstrom T., Norrving B., Schtchkute A. Cerebrovasc.
Dis. 2007; 23: 229-41
Cele na rok 2015:
Do roku 2015 co najmniej 70% osób
spośród tych którzy przeżyli udar uzyska
w ciągu
3 miesięcy samodzielność w
czynnościach codziennych (ADL)
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006 on European Stroke Strategies
Kjellstrom T., Norrving B., Schtchkute A. Cerebrovasc. Dis. 2007; 23: 229-41
Basic Requirements
Following acute treatment it is essential to avoid bedrest and to mobilize
patients as early as possible. At the start of rehabilitation, every patient
should have access to rehabilitation services. For maximum effectiveness,
this includes the availability of a multidisciplinary stroke team. When
awake and medically stable, a patient should be assessed by a team of
neurologically trained professionals using a standard check-list to
identify problems. This
assessment includes not only motor functions but also cognitive and
emotional /behavioural domains known to be frequently affected by
stroke. In addition, the patient’s general health, nutritional and
continence status, any concomitant diseases and special needs should be
considered. As soon as appropriate, the patient should take part in goal-
planning involving all the rehabilitation professionals. It is essential to
formulate goals that are achievable and include the personal and social
domains. According to a patient’s needs, he/she should:
• receive relevant interventions
• be reassessed, and
• take part in goal-planning.
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006 on European Stroke
Strategies
Kjellstrom T., Norrving B., Schtchkute A. Cerebrovasc.
Dis. 2007; 23: 229-41
The Roles of Patients and Their Families
Carers are recognized as important contributors in the
rehabilitation process. Rehabilitation should, therefore,
be planned in close collaboration with the patient and the
carers. They should take part in the rehabilitation process
which is centred on the patient’s own goals.
For this to be effective, patients and their carers should
be provided with medical and nursing information at all
levels and for all phases of rehabilitation. They should receive
written education materials and support from professionals
as well as lay organizations (wherever appropriate)
to improve their abilities to cope with the impairment
of function and their participation in the process.
Thus it is essential that patients and their carers are satisfied
with the information received both in hospital and
outside from outpatient settings, community health services
and patients’ organizations.
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006 on European Stroke Strategies
Kjellstrom T., Norrving B., Schtchkute A. Cerebrovasc. Dis. 2007; 23: 229-41
Multidisciplinary Rehabilitation Team
To be most effective, rehabilitation requires the intervention
of a multidisciplinary team consisting of a physician
trained in stroke medicine, a nurse experienced and
trained in stroke rehabilitation, a physiotherapist, an occupational
therapist, and a speech therapist trained and
experienced in stroke rehabilitation. Some patients will
require the intervention of a social worker, who should
also be considered part of the team. Assessment by a neuropsychologist
should be available when needed. Other
professionals, such as a dietitian and orthoptician, can be
included as necessary.
In some settings, including smaller hospitals, conditions
may dictate that one or more of the professionals
fulfil more than one of these roles and multidisciplinary
efforts are shared among the professional members of the
team. But this should not impede or delay achievement of
the overall goals as defined by the needs of the patients
and their families.
Nowoczesna
rehabilitacja
Helsingborg Declaration 2006 on European Stroke Strategies
Kjellstrom T., Norrving B., Schtchkute A. Cerebrovasc. Dis. 2007; 23: 229-41
Interventions
The selection of methods and techniques should be
based on evidence as far as possible and follow available
international or national guidelines.
Such interventions are usually specific, targeted and
task-oriented. They should also be relevant to the patient,
that is, in accordance with the patient’s own goals, and
take account of appropriate social dimensions for learning
and practice.
Measures should include rehabilitation of emotional
responses and behavioural skills with a special focus on
social integration and restoration of cognitive abilities.
Where applicable, interventions for the restoration of
professional working abilities should be included as early
as possible.
When medically feasible, rehabilitation should include
training sessions to improve physical fitness.
Formal training sessions with the multidisciplinary
team should be supplemented by training for carers and
volunteers, as directed by health professionals.
Team-based training will in most cases be finished
within the first year following stroke. Some patients may
need later reassessment by a multidisciplinary team,
which should be provided. Often further improvements
in function and social participation can be achieved with additional rehabilitation.
Nowoczesna
rehabilitacja
Sacco RL, Adams R, Albers G, Alberts MJ,
Benavente O, Furie K, Goldstein LB,Gorelick P,
Halperin J, Harbaugh R, Johnston SC, Katzan I,
Kelly-Hayes M, KentonEJ, Marks M, Schwamm
LH, Tomsick TGuidelines for prevention of
stroke in patients with ischemic stroke or
transient ischemic attack: a statement for
healthcare professionals from the American
Heart Association/American Stroke Association
Council on Stroke: co-sponsored by the Council
on Cardiovascular Radiology and Intervention:
the American Academy of Neurology affirms the
value of this guideline.
Circulation. 2006 Mar 14;113(10):e409-49.
Nowoczesna
rehabilitacja
Sacco RL, Circulation. 2006,113(10):e409-49.
G. Physical Activity
Recommendation
For patients with ischemic stroke or TIA who
are capable of engaging in physical activity, at
least 30 minutes of moderate-intensity
physical exercise most days may be considered
to reduce the risk factors and comorbid
conditions that increase the likelihood of
recurrence of stroke (Class IIb, Level of
Evidence C). For those individuals with
disability after ischemic stroke, a supervised
therapeutic exercise regimen is recommended
Nowoczesna
rehabilitacja
Gordon NF, Gulanick M, Costa F, Fletcher G,
Franklin BA, Roth EJ, Shephard T. Physical
activity and exercise recommendations
for stroke survivors: an American Heart
Association scientific statement from the
Council on Clinical Cardiology,
Subcommittee on Exercise, Cardiac
Rehabilitation, and Prevention; the
Council on Cardiovascular Nursing; the
Council on Nutrition, Physical Activity,
and Metabolism; and the Stroke Council.
Circulation. 2004 Apr 27;109(16):2031
Nowoczesna
rehabilitacja
Gordon NF, Circulation 2004;109(16):2031
3 major rehabilitation goals for the
stroke patient are:
1.
preventing complications of prolonged
inactivity,
2.
decreasing recurrent stroke, and
cardiovascular events, and
3.
increasing aerobic fitness.
Nowoczesna
rehabilitacja
Schettino LF, Adamovich SV, Poizner
H.Effects of object shape and visual
feedback on hand configuration during
grasping. Exp Brain Res. 2003
Jul;151(2):158-66.
Merians AS, Poizner H, Boian R, Burdea G,
Adamovich S. Sensorimotor training in a
virtual reality environment: does it improve
functional recovery poststroke?
Neurorehabil Neural Repair. 2006
Jun;20(2):252-67.
Nowoczesna
rehabilitacja
Virtual Reality (VR)
– rzeczywistość wirtualna
Udawanie świata realnego przy zastosowaniu
wzajemnego oddziaływania człowiek – maszyna.
Wyświetlacz wzrokowy zamontowany na głowie
lub monitorze, urządzenie śledzące ruch,
urządzenie wykrywające siłę, lub
wzmocnione sprzężenie czuciowe
(reakcja jest bardziej widoczna i wybiórcza niż
w świecie rzeczywistym)
Nowoczesna
rehabilitacja
Virtual Reality (VR)
– rzeczywistość wirtualna
wirtualny nauczyciel
rękawice cyfrowe
odmiana bio-feedbacku
zdobyte punkty nagrodą za zdrowienie
ruch w rzeczywistości wirtualnej uogólnia się na
rzeczywistość
ćwiczenia bardziej skuteczne niż w świecie
rzeczywistym
Wykorzystanie
plastyczności mózgu
Pascual-Leone A, Amedi A, Fregni F, Merabet
L. The plastic human brain cortex.
Annu Rev Neurosci. 2005;28:377-401.
Classen J, Liepert J, Wise SP, Hallett M,
Cohen LG.Rapid plasticity of human
cortical movement representation
induced by practice. J Neurophysiol. 1998
Feb;79(2):1117
Sawaki L, Cohen LG, Classen J, Davis BC,
Butefisch CM.Enhancement of UDP -
U
se-
D
ependent
P
lasticity by D-amphetamine.
Neurology. 2002 Oct 22;59(8):1262-4.
UDP
UDP -
U
se-
D
ependent
P
lasticity
Ćwiczenia wyzwalają plastyczność
mózgu zależną od treningu
Ćwiczenia prowadzą do zapamiętania
strategii adaptacyjnych
UDP zmniejsza się z wiekiem
Prezentacja nagrania osoby wykonującej
ćwiczenia wywołuje zmiany plastyczne
w korze mózgowej obserwatora
Nowoczesna
rehabilitacja
Duncan PW, Zorowitz R, Bates B,
Choi JY, Glasberg JJ, Graham GD,
Katz RC, Lamberty K, Reker D.
Management of Adult Stroke
Rehabilitation Care: a clinical
practice guideline. Stroke. 2005
Sep;36(9):e100
Nowoczesna
rehabilitacja
Duncan PW, Stroke. 2005, 36(9):e100
Recommendation Source QE Overall Qual. R
____________________________________________________________
1. Early initiation of Therapy Cifu and Stewart, 1999 I Good
A
Ottenbacher and Jannell,
1993
2. Intensity of therapy Kwakkel et al, 1999; I Fair
B
Langhorne et al, 1996;
Richards et al, 1993;
Sivenius et al, 1985;
Smith et al, 1981;
van der Lee and Snels,
2001
Nowoczesna
rehabilitacja
Cifu DX, Stewart DG. Factors affecting
functional outcome after stroke: a
critical review of rehabilitation
interventions. Arch Phys Med Rehabil.
1999 May;80 (5 suppl 1):S35-9.
Ottenbacher KJ, Jannell S. The results of
clinical trials in stroke rehabilitation
research. Arch Neurol. 1993
Jan;50(1):37-44.
Nowoczesna
rehabilitacja
Early Supported Discharge Trialists.
Services for reducing duration of
hospital care
for acute stroke patients.
Cochrane Database of Systematic
Reviews 2005, Issue 2.
Cochrane Database of Systematic
Reviews 2007 Issue 1
Nowoczesna
rehabilitacja
John W. Krakauer, Pietro Mazzoni, Ali
Ghazizadeh, Roshni Ravindran, Reza
Shadmehr.
Generalization of Motor
Learning
Depends on the History of Prior Action.
Curr Opin Neurol. 2006 Feb;19(1):84-90.
Dept of Neurology, Columbia University
College of Physicians and Surgeons, New
York, New York, United States of America
Nowoczesna
rehabilitacja
Hummel FC, Cohen LG. Drivers of brain
plasticity. Curr Opin Neurol. 2005
Dec;18(6):667-74.
Human Cortical Physiology Section,
National Institute of Neurological
Disordersand Stroke, National Institutes
of Health, Bethesda, MD 20817, USA.
NOWOCZESNA REHABILITACJA
POUDAROWA
Potrzeby
?
Nowoczesna
rehabilitacja poudarowa
Nowoczesna
rehabilitacja poudarowa
Przyjmując dane statystyczne biorące
pod uwagę wszystkie rodzaje udarów,
określające śmiertelność w ciągu
pierwszego miesiąca na ok. 30%
otrzymamy wyliczenie:
ok. 10% opuszcza szpital bez
ubytków,
ok. 60% chorych pozostaje po udarze
z trwałymi objawami ogniskowego
uszkodzenia OUN
- ci ostatni wymagają rehabilitacji.
Nowoczesna
rehabilitacja poudarowa
Osoby które przeżyły udar z trwałymi
objawami uszkodzenia OUN najczęściej
cechują się:
obecnością niedowładu połowiczego,
zmniejszeniem samodzielności w
czynnościach codziennych,
część z nich cierpi ma trudności z
kontaktem słownym,
niemało z nich wykazuje objawy depresji.
Nowoczesna
rehabilitacja poudarowa
Co rozumiemy jako
nowoczesną rehabilitację
poudarową?
1. Czy są to najnowsze doniesienia z
dziedziny rehabilitacji neurologicznej i
neurorehabilitacji (w tym metoda CIT -
Constraint-Induced Movement Therapy),
plastyczności mózgu itp?
2. Czy jest to zastosowanie komputera,
zwłaszcza w kinezyterapii i rehabilitacji
zaburzeń poznawczych?
Nowoczesna
rehabilitacja poudarowa
Co rozumiemy jako nowoczesną rehabilitację poudarową?
c.d.
3. Zastosowanie najnowszych metod obrazowania układu
nerwowego (PET, fMRI), komputeryzacji i badań neuro-
fizjologicznych, dla wzbogacenia diagnostyki,
wypracowania nowych metod rehabilitacji i oceny
jej wyników?
4. Czy oznaką nowoczesności jest intensyfikacja ćwiczeń?
5. Czy niezbędne jest zastosowanie nowych metod
obiektywnej oceny skuteczności rehabilitacji?
6. Jak bardzo powinien być rozbudowany zespół
rehabilitacyjny?
NOWOCZESNA REHABILITACJA
POUDAROWA
Cele
?
Nowoczesna
rehabilitacja poudarowa
Nowoczesna
rehabilitacja poudarowa
C e l e: ?
1.
Poprawa samodzielności
2.
Poprawa sprawności kończyn
3.
Lokomocja
4.
Poprawa sprawności ogólnej
5.
Poprawa komunikacji słownej
6.
Poprawa jakości życia
Nowoczesna rehabilitacja poudarowa
Ustalenie celów rehabilitacji
1. Cele uzgodnione z pacjentem
2. Cele uzgodnione z rodziną
3. Współpraca i współudział
rodziny
i / lub opiekunów
Nowoczesna
rehabilitacja poudarowa
Jak osiągnąć założone c e l e ?
Nowoczesna
rehabilitacja poudarowa
Dwie strategie postępowania:
1. Terapia oparta na objawach
(ang. facilitation - impairment-based
approach)
2. Terapia oparta na zadaniach
(ang. task-oriented - disability-
focused approach)
Nowoczesna
rehabilitacja poudarowa
1.
Terapia oparta na objawach.
Najczęściej stosowane metody ćwiczeń po
udarze:
1. Metoda Kabata - PNF
(Proprioceptive neuromuscular facilitation)
2. Metoda Bobath - NDT
(Neurodevelopmental treatment)
3. Ćwiczenia koordynacyjno-równoważne wg Frankela
4. Bio-feed-back
Nowoczesna
rehabilitacja poudarowa
1.
Terapia oparta na objawach.
Spastyczność
Dysfunkcja neurogenna pęcherza
moczowego
Zaburzenia utrzymania postawy ciała i
równowagi
Nowoczesna
rehabilitacja poudarowa
Dwie strategie postępowania:
2.
Terapia oparta na zadaniach (ang. task-
oriented - disability-focused approach)
W ostatnich latach ukazały się doniesienia
wskazujące na skuteczność treningu
kondycyjnego (ang. aerobic exercise) po
udarze. Wykazano, że przy zachowaniu ścisłych
kryteriów kwalifikacji do wysiłku aerobowego
można uzyskać poprawę wydolności chorych.
Trening ten musi jednak trwać co najmniej kilka
tygodni, a najlepiej kilka miesięcy.
Nowoczesna
rehabilitacja poudarowa
Aerobic exercise
1. MacKay-Lyons MJ, Howlett J. Exercise
capacity and cardiovascular adaptations to
aerobic training early after stroke. Top Stroke
Rehabil. 2005 Winter;12(1):31-44
2. Macko RF, Ivey FM, Forrester LW. Task-
oriented aerobic exercise in chronic
hemiparetic stroke: training protocols and
treatment effects. Top Stroke Rehabil. 2005
Winter;12(1):45-57
Nowoczesna
rehabilitacja poudarowa
C e l e: ?
1.
Poprawa samodzielności
2.
Poprawa sprawności kończyn
3.
Lokomocja
4.
Poprawa sprawności ogólnej
5.
Poprawa komunikacji słownej
6.
Poprawa jakości życia
Wskaźnik Funkcjonalny „Repty”
Samoobsługa
:
1. Spożywanie posiłków
2. Dbałość o wygląd zewnętrzny i higienę osobistą
3. Kąpiel
4. Ubieranie g. części ciała
5. Ubieranie d. części ciała
6. Toaleta
Kontrola zwieraczy : 7. Oddawanie moczu
8. Oddawanie stolca
Mobilność : 9. Przechodzenie z łóżka na krzesło i z powrotem
10. Siadanie na muszli klozetowej
11. Wchodzenie pod prysznic lub do wanny

Wskaźnik Funkcjonalny „Repty”
c.d.
Lokomocja : 12. Chodzenie lub jazda na wózku inwalidzkim
13. Schody
Komunikacja : 14. Zrozumienie słowne lub wizualne
15. Mowa werbalna
Punktacja :
7 - pełna niezależność
5 - umiarkowana zależność
3 - wymagana pomoc
1 - całkowita zależność
Nowoczesna
rehabilitacja poudarowa
Jak uzyskać poprawę samodzielności w
czynnościach
samoobsługi?
1.
Terapia zajęciowa
2.
Kinezyterapia
3.
Metoda CIT
4.
Pomocniczy sprzęt rehabilitacyjny i
ortopedyczny
5.
Adaptacja mieszkania
Nowoczesna
rehabilitacja poudarowa
Jak uzyskać poprawę lokomocji?
1. Kinezyterapia
2. Tor do nauki chodzenia
z różnymi
nawierzchniami
3.
Bieżnia ruchoma z odciążeniem
4.
Funkcjonalna Elektro-Stymulacja (FES)
5. Musical motor feedback (MMF)
6. Pomocniczy sprzęt rehabilitacyjny i ortopedyczny
Nowoczesna
rehabilitacja
Jak uzyskać poprawę
utrzymania postawy ciała i równowagi?
1. Kinezyterapia
2. Tor do nauki chodzenia z przeszkodami
3. Bieżnia ruchoma z odciążeniem
4. Musical motor feedback (MMF)
5. Ćwiczenia koordynacyjno-równoważne
(Frankel)
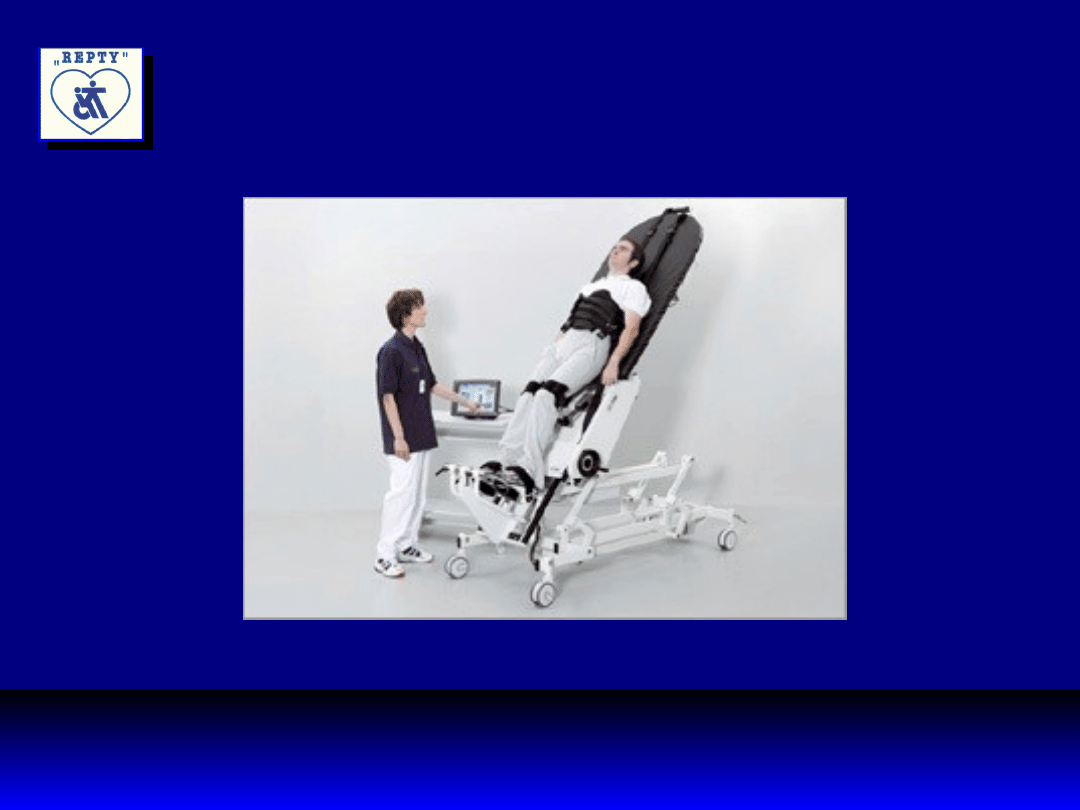
Nowoczesna
rehabilitacja
Najnowsze urządzenia:
Lokomat System
Erigo - Tilt table for the mobilization
Lokolift - Electronically controlled body weight
support system

Nowoczesna
rehabilitacja
Lokomat
Nowoczesna
rehabilitacja
Erigo
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Kwakkel G., Wagenaar R.C., Koelman T.W. et al.
1997. Effects of intensity of rehabilitation after
stroke: a research synthesis. Stroke; 28, 8: 1550-
6.
Van Peppen R.P., Kwakkel G., Wood-Dauphinee S.,
Hendriks H., Van der Wees P., Dekker J. The
impact
of physical therapy on functional outcomes after
stroke: what's the evidence? Clin Rehabil. 2004
Dec;18(8):833-62.
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Van Peppen R.P., Kwakkel G., Wood-Dauphinee S.,
Hendriks H., Van der Wees P., Dekker J. The impact of
physical therapy on functional outcomes after stroke:
what's the evidence? Clin Rehabil. 2004 Dec;18(8):833
In total, 151 studies were included in this systematic
review; 123 were randomized controlled trials (RCTs)
and 28 controlled clinical trials (CCTs).
CONCLUSIONS: This review showed small to large effect
sizes for task-oriented exercise training, in particular
when applied intensively and early after stroke onset.
In almost all high-quality RCTs, effects were mainly
restricted to tasks directly trained in the exercise
program.
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Schauer M., Mauritz K.H. 2003. Musical Motor
Feedback (MMF) in walking hemiparetic
stroke patients: randomized trials of gait
improvement. Clin. Rehabil. 17(7): 713-22
Pang M.Y., Eng J.J., Dawson A.S. et al. 2005. A
community-based fitness and mobility
exercise program for older adults with
chronic stroke: a randomized, controlled
trial. J Am Geriatr Soc.; 53(10): 1667-74
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Macko R.F., Ivey F.M., Forrester L.W. et al. 2005.
Treadmill exercise rehabilitation improves
ambulatory function and cardiovascular fitness in
patients with chronic stroke:
a randomized, controlled trial. Stroke; 36(10):
2206-11
Eich H.J., Mach H., Werner C., Hesse S. Aerobic
treadmill plus Bobath walking training improves
walking in subacutestroke: a randomized controlled
trial. Clin Rehabil. 2004 Sep;18(6):640-51
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Hesse S., Werner C., Bardeleben A., Barbeau H. Body
weight-supported treadmill training after
stroke.
Curr Atheroscler Rep. 2001 Jul;3(4):287-94
Peurala S.H., Tarkka I.M., Pitkanen K., Sivenius
J. The effectiveness of body weight-supported gait
training and floor walking inpatients with chronic
stroke. Arch Phys Med Rehabil. 2005
Aug;86(8):1557-64
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia: Tele-rehabilitacja
Piron L., Tonin P., Trivello E., Battistin L.,
Dam M. Motor tele-rehabilitation in
post-stroke patients Med Inform
Internet Med. 2004 Jun;29(2):119-25.
Dept of Neurorehabilitation, San
Camillo Hospital, via Alberoni 70, 30011
Lido di Venezia, Italy.
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Hesse S., Werner C., Pohl M., Rueckriem S.,
Mehrholz J., Lingnau M.L. Computerized arm
training improves the motor control of the
severely affected arm after stroke: a single-
blinded randomized trial in two
centers. Stroke. 2005 Sep;36(9):1960-6
Hesse S., Schmidt H., Werner C., Bardeleben
A. Upper and lower extremity robotic devices
for rehabilitation and for studyingmotor
control. Curr Opin Neurol. 2003 Dec;16(6):705-
10
Nowoczesna
rehabilitacja poudarowa
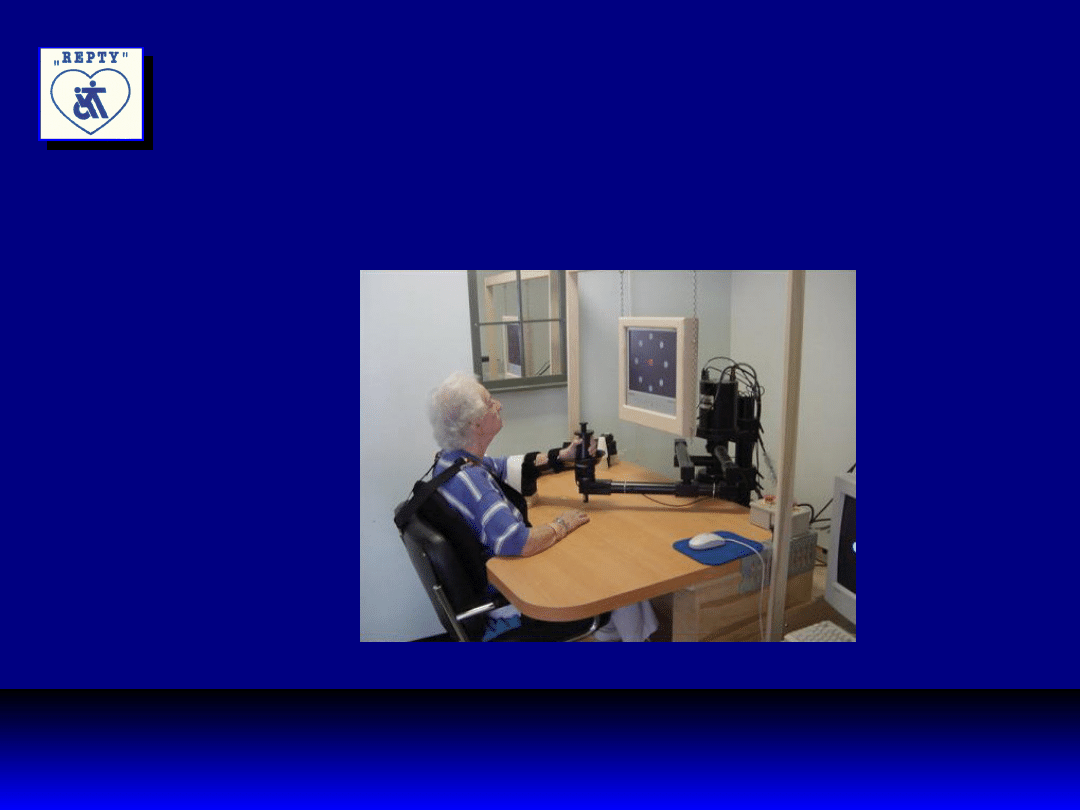
Najnowsze doniesienia: robotics
Krebs H.I., Ferraro M., Buerger S.P., Newbery M.J.,
Makiyama A., Sandmann M., Lynch D.,Volpe
B.T., Hogan N. Rehabilitation robotics: pilot
trial of a spatial extension for MIT-MANUS. J
Neuroengineering Rehabil. 2004 Oct 26;1(1):5.
Massachusetts Institute of Technology,
Mechanical Engineering Dept.,Cambridge
Burke Rehabilitation Hospital, White Plains, NY, Spaulding
(MA), Rhode Island (RI), Osaka Prefectural (Japan),
Helen Hayes (NY) Rehabilitation Hospitals,
Baltimore (MD) Veterans Administration Medical Center,
Cleveland (OH) Veterans Administration Medical Center.
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia: robotics
Gabor Fazekas, Zoltan Denes, Eszter Herczeg
et al.
REHAROB. National Institute for medical
Rehabilitation.
Budapest.
Nowoczesna
rehabilitacja poudarowa
MIT MANUS
Nowoczesna
rehabilitacja poudarowa
Najnowsze doniesienia:
Burgar C.G., Lum P.S., Shor P.C., Van der
Loos, H.F.M. Development of robots for
rehabilitation therapy: the Palo Alto VA /
Stanford experience. J Rehab Res Dev,
2000; 36: 663-673
Nowoczesna
rehabilitacja poudarowa
Teasell R.W., Foley N.C., Bhogal S.K., Speechley
M.R.
An evidence-based review of stroke
rehabilitation. Top Stroke
Rehabil. 2003 Spring;10(1):29-58
Teasell R.W., Kalra L. What's new in stroke
rehabilitation:
back to basics. Stroke. 2005 Feb;36(2):215-7

Nowoczesna
rehabilitacja poudarowa
http://www.wcnr2006.com/home.htm
http://www.wfnr.co.uk/
www.isprm.org/
14, 2007
Nowoczesna
rehabilitacja poudarowa
http://www.wcnr2006.com/home.htm
Session 7D - Tele-rehabilitation
• Tele-rehabilitation: Clinical,
Technological and
Socio-economic Aspects. Lamberto
Piron (Italy)
• Experimental Projects of Upper Limb
Telerehabilitation. Mauro Zampolini
(Italy)
• Tele-stroke and tele-cognitive
rehabilitation:
A tribute to Prof. Alan Tam. Margaret
Mak
(Hong Kong)
Nowoczesna
rehabilitacja poudarowa
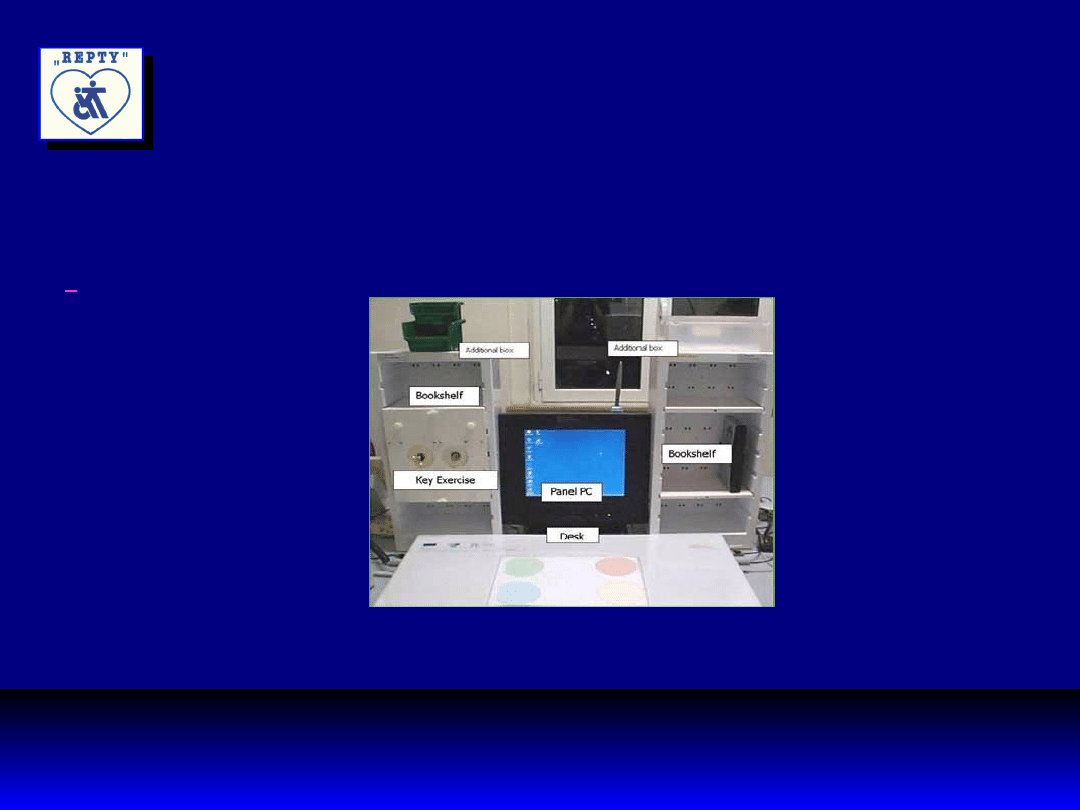
HCAD – Home Care Activity Desk
Nowoczesna
rehabilitacja poudarowa
4th WCNR Hong Kong, 12-16 February 2006
Main Symposium III (15 February, Wednesday)
Rehabilitation: Human / Machine Interface
1. Introduction (Chair): Prof. Michael Weinrich, National
Institutes of Health (USA)
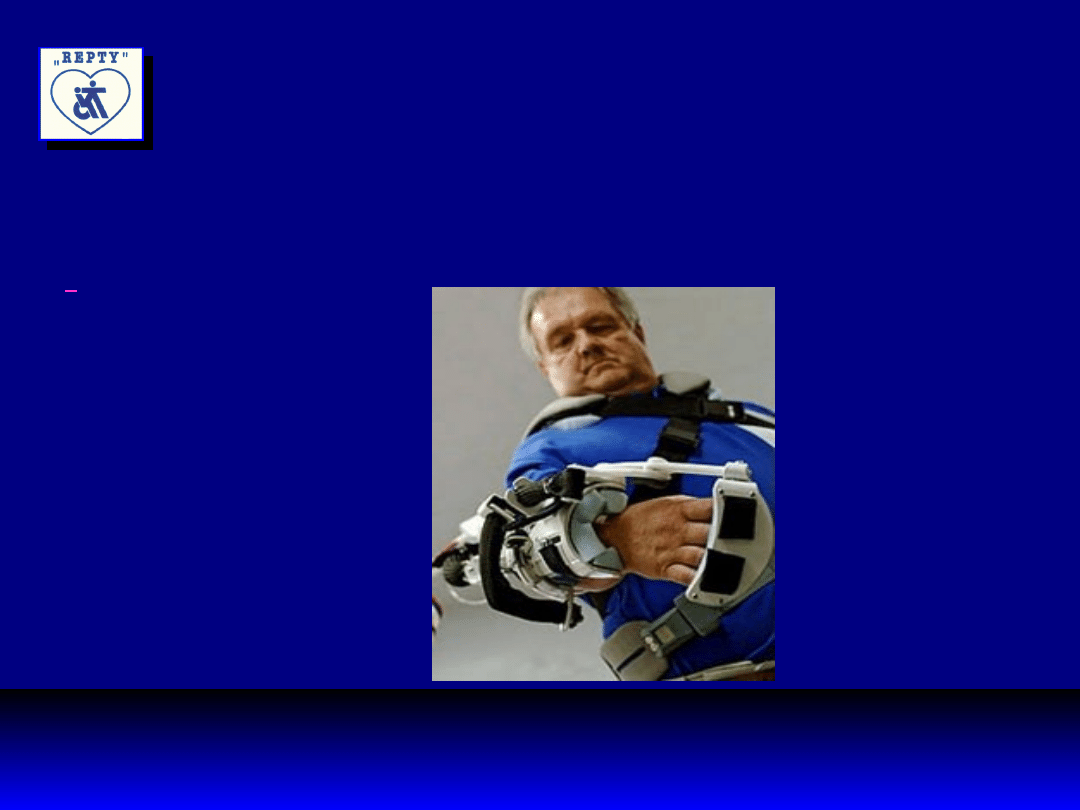
2. The development of a Wearable Robot (RUPERT) for
Neural Rehabilitation Dr. Jiping He, Arizona State
University (USA)
RUPERT - Robotic Upper Extremity Repetitive Therapy
3. Rehabilitation Robotics and Stroke. Dr. Hermano Igo
Krebs, Massachusetts Institute of Technology (USA)
Nowoczesna
rehabilitacja poudarowa
RUPERT
Nowoczesna
rehabilitacja poudarowa
http://www.wcnr2006.com/home.htm
4th WCNR Hong Kong, 12-16 February 2006
Session 1D - Update on Stroke Rehabilitation I
•
Evidence based review on stroke rehabilitation.
EBM
Karl Heinz Mauritz (Germany)
•
Functional Outcomes in Stroke in-patients.
Haim Ring (Israel)
Nowoczesna
rehabilitacja poudarowa
http://www.wcnr2006.com/home.htm
4th WCNR Hong Kong, 12-16 February 2006
Session 7A - Quality of Life Issues & ICF
1. The Child and Adolescent after Severe Traumatic
Brain Injury: Quality of Life and Functional Outcomes.
Lucia Braga (Brazil)
2. The Latest Development of Measurement in Quality
of Life after Stroke. Józef Opara (Poland)
3. ICF Classification in Neurorehabilitation: Guiding
the Multidisciplinary Care. Matilde Leonardi (Italy)
Nowoczesna
rehabilitacja poudarowa
Czasopisma
IF
Archives of Physical Medicine and Rehabilit
ation
1,7
1,144
Journal of Rehabilitation Medicine
1,6
NeuroRehabilitation
0,561
Neurorehabilitation and Neural Repair
1.850
Scandinavian Journal of Rehabilitation
Medicine
1,333
Nowoczesna
rehabilitacja poudarowa
Podręczniki
QoL
after Stroke
International Classification of
Functioning, Disability and Health –
ICIDH 2
Geneva, WHO 2001
ICF
.
Body function →
Activities at the individual level →
Participation
Algorytm postępowania
rehabilitacyjnego
Diagnostyka
Ocena rokowania
Ocena funkcjonalna
Planowanie rehabilitacji
Realizacja
Nowoczesna
rehabilitacja poudarowa
Diagnostyka
1.
Analiza chodu
2.
Posturometria i stabilometria
3.
EMG
4.
MEP
5.
TCMS
Nowoczesna
rehabilitacja poudarowa
Diagnostyka i terapia:
TCMS
Talelli P,
Greenwood RJ, Rothwell JC. Arm function
after stroke: Neurophysiological correlates and
recovery mechanisms assessed by transcranial
magnetic stimulation. Clin Neurophysiol. 2006 Apr 2
TransCranial Magnetic Stimulation for Stroke
Rehabilitation. Preliminary Study. This study is
currently recruiting patients.
Verified by National Institutes of Health Clinical
Center (CC) October 7, 2005. Sponsored by:
National Institute of Neurological Disorders and Stroke
(NINDS)
Information provided by: National Institutes
of Health Clinical Center (CC). Clinical Trials. gov
Identifier: NCT00050128
Nowoczesna
rehabilitacja poudarowa
Nieinwazyjna stymulacja
korowa:
1.
rTMS – powtarzana przezczaszkowa
stymulacja magnetyczna
2.
tDCS – transcranial Direct Current
Stimulation
stymulacja prądem stałym
Nowoczesna
rehabilitacja poudarowa
1.
rTMS – powtarzana przezczaszkowa
stymulacja magnetyczna
a) niskiej częstotliwości: 0,9 – 1 Hz
b) wysokiej częstotliwości: 5 – 20 Hz
c) stymulacja wiązką theta przez 20-190
sek.
Huang YZ, Edwards MJ, Rounis E, Bhatia KP, Rothwell JC.
Theta burst stimulation of the human motor cortex. Neuron.
2005 Jan 20;45(2):201-6.
Nowoczesna
rehabilitacja poudarowa
rDCS - przezczaszkowa stymulacja prądem
stałym
Indukuje ogniskowe, długotrwałe,
odwracalne zmiany pobudliwości korowej
Może służyć do modulacji aktywności
korowej
i parametrów behawioralnych w korze
ruchowej,
somatosensorycznej, wzrokowej i
przedczołowej
Nowoczesna
rehabilitacja poudarowa
rDCS - przezczaszkowa stymulacja prądem
stałym
Elektrody powierzchniowe o pow. 25-35 cm²
Stymulacja anodowa zwiększa pobudliwość
kory
Stymulacja katodowa zmniejsza pobudliwość
kory
Czas trwania stymulacji: 30 min
Czas trwania modulacji czynności kory: ½ +
1,5 h
Nowoczesna
rehabilitacja poudarowa
Stymulacja kory mózgowej w
neurorehabilitacji
Poprawa sprawności ruchowej
Poprawa koordynacji wzrokowo-ruchowej
Poprawa ruchów precyzyjnych palców
Poprawa pamięci operacyjnej
Konsolidacja pamięci deklaratywnej
zależnej
od snu
Nowoczesna
rehabilitacja poudarowa
Stymulacja somatosensoryczna
1.
PNS (Percutaneous Neuro-
Stimulation)
- stymulacja nerwów obwodowych
2.
INB (Ischaemic Nerv Block)
- niedokrwienna blokada nerwów
Napompowanie mankietu sfigmomanometru
na przedramieniu powyżej ciśnienia
skurczowego
Nowoczesna
rehabilitacja poudarowa
Stymulacja somatosensoryczna
3.
Znieczulenie
a) miejscowe
b) przewodowe
Przejściowe znieczulenie zdrowej ręki powoduje
poprawę sprawności ruchowej i
somatosensorycznej
drugiej ręki
Nowoczesna
rehabilitacja poudarowa
Stymulacja
somatosensoryczna
Bjorkman A, Rosen B, Lundborg G. Acute
improvement of hand sensibility after
selective ipsilateral cutaneous
forearm anaesthesia. Eur J Neurosci.
2004 Nov;20(10):2733-6.
Nowoczesna
rehabilitacja poudarowa
Stymulacja somatosensoryczna
Muellbacher W, Richards C, Ziemann U,
Wittenberg G, Weltz D, Boroojerdi B,
CohenL, Hallett M. Improving hand
function in chronic stroke. Arch Neurol.
2002 Aug;59(8):1278-82.
Znieczulenie włókien ruchowych splotu
ramiennego prowadzi do poprawy
sprawności ręki
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
- Slide 59
- Slide 60
- Slide 61
- Slide 62
- Slide 63
- Slide 64
- Slide 65
- Slide 66
- Slide 67
- Slide 68
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
Wyszukiwarka
Podobne podstrony:
Diagnostyka funkcjonalna, Fizjoterapia - Kinezyterapia
ANALIZA FUNKCJONALNA PACJENTA wykład 1 23, FIZJOTERAPIA, Diagnostyka funkcjonalna
diagnostyka funkcjonalna i programowanie rehabilitacji wykład 1, fizjoterapia
Plastyczność mózgu, Studia - materiały, referaty itd, Fizjoterapia, Diagnostyka funkcjonalna
Diagnostyka funkcjonalna w rehabilitacji i fizjoterapii
Diagnostyka funkcjonalna dla potrzeb fizjoterapeuty(1), studia fizjoterapia, fizjoterapia
Badanie nerwów czaszkowych, Studia - materiały, referaty itd, Fizjoterapia, Diagnostyka funkcjonalna
Podzial Plastycznosci mozgu, Studia - materiały, referaty itd, Fizjoterapia, Diagnostyka funkcjonaln
TEST ODCINKA PIERSIOWEGO I LĘDŹWIOWEGO, Studia - materiały, referaty itd, Fizjoterapia, Diagnostyka
Zagadnienia egzaminacyjne - diagnostyka funkcjonalna w neurologii
Lista osób dopuszczonych na egz zerowy Diagnostyka, Fizjoterapia, DIAGNOSTYKA FUNKCJONALNA
Wskaźnik funkcjonalny „Repty”, Fizjoterapia, neurologia
więcej podobnych podstron