
PSYCHOSOMATIC MEDICINE AND THE
PSYCHOLOGY OF THE SOMATICLY ILL -
practical
Magdalena Lazarewicz
Dept. of Medical Psychology,
Warsaw Medical University
magda.lazarewicz@gmail.com
Psychological
consequences of
somatic disease

Past…
Main Schools of Psychology
Psychology + Medicine Disciplines
Stress
Situational risk factors in somatic disease
Personality risk factors in somatic disease
Type A behaviour as a risk factor in
somatic disease

Literature concerning topics discussed
so far
Wrzesniewski, K., Skuza, B. (2004).
Psychosomatic Medicine and The
Psychology of the somatically ill. Selected
issues. A Textbook for Medical Students.
Introduction & PART I, pp. 1-38.
Ogden, J. (2001). Chapter 10. Stress. In:
Health Psychology: A textbook. pp. 231-254.
Future…
Psychological consequences of somatic
disease
Psychological Aspects of Treatment of the
Somatic Patient
Selected Aspects of Psychosomatic Diagnosis
• Role-playing +
Essay
• Test

Today…
Psychological consequences of somatic
disease
–
Effects of disease on human functioning
–
Illness Cognitions (IC)
–
Attitudes Towards Illness (ATI)

Indirect effects of disease on
human functioning 1
How does being ill influence your behaviour?
How does it influence your everyday life?
What is the worst thing about being ill? What do you
concentrate on
(e.g. symptoms, diagnosis, not being able to
achieve your goals, relaxing and watching TV)?
How do you usually feel when you’re ill?
Have you ever been to the hospital as a patient? How
did you feel?

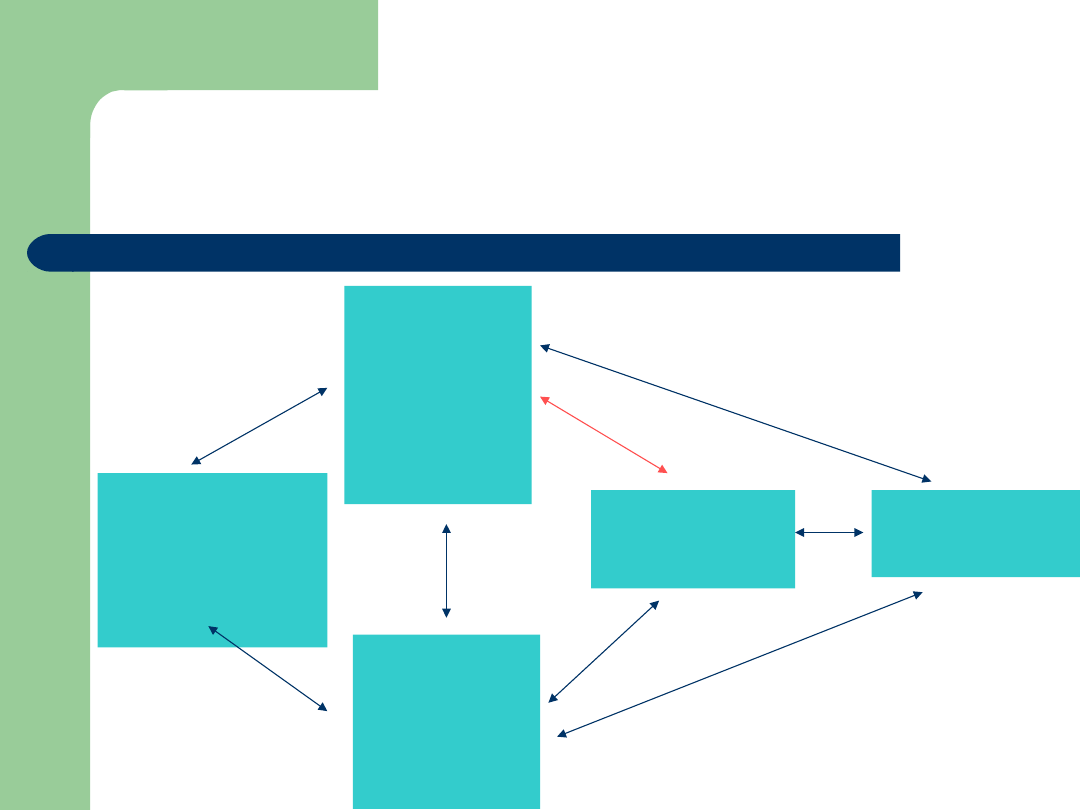
Indirect effects of disease on human functioning
2
–
somatic disease as a stressful situation
Discomforts of
illness
•Pain
•Breathlessness
•Itchiness
•Chronic dizziness
•Vomiting
•
Modified hierarchy of
incoming information
•
Impairment of cognitive
processes
•
Impairment of affective
processes
•
Decrease in general
mental efficiency (memory
functions, attention and
learning ability)
•
Emotional disturbances
(depression, irritability,
impulsiveness, anxiety)
•
Activity impairment
(conscious and organized
goal-directed behaviour)
often
conceptualis
ed as a
disease
itself
Limitations
(mainly in
chronic diesese)
•
Difficulties with walking and eating
•
Diet
•
Difficulties with personal hygiene
and dressing
•
Giving up old habits: smoking,
coffee, strong tea, alcohol
Hospitalizati
on
Disruption of famiy
and profesional
roles
Indirect effects of disease on
human functioning 3 -
HOSPITALIZATION
„I’M GOING TO THE HOSPITAL!!!”
„I’M VERY VERY SICK!”

Indirect effects of disease on
human functioning 4 –
HOSPITALIZATION
Interruption of ongoing social relationships
New environment – new people:
–
Hospital staff (discipline, obey orders)
–
Other patients (different habits, interests, customs as
well as their suffering and severity of illness)
Specific diagnostic and therapeutic procedures
–
Undressing in public for physical examination
–
Routine collections of blood samples
–
Invasive diagnostic procedures

Indirect effects of disease on
human functioning 5 –
HOSPITALIZATION
Hospital schedule / rules / regulations
(e.g.
early mornings)
Depersonalization
(PERSON as a „CASE from room 12”,
„kidney stone case”, „interesting case”)
Being treated like a child
Sensory deprivation

Indirect effects of disease on
human functioning 6
Disruption of family
–
Disruption of the previous rhythm of family life
–
New roles
–
Dependence
Disruption of professional roles
–
Economic deterioration
–
Lowering social status
–
Giving up goals and ambitions

Possible responses to the
situation of being ill
How the patient responds to the situation of
being ill will depend not only on objective
physical and psychosocial threat but also on the
subjective appraisal of the situation and
personal concepts of health and illness.
Illness may be viewed (appraised) as:
–
Obstacle
–
Loss
(e.g. invalidism)
–
Relief
(e.g. illnes as an excuse)
–
Benefit
(material
<e.g. pensions, reparations>
or psychological
<extra care and support>
advantages)
–
Value
(e.g. deeply religious people – metaphysical value
ascribed to suffering)
Personal concepts of health and
illness
What
does it
mean to
be
healthy?
What
does it
mean to
be ill?

What does it mean to be
healthy?
Health
as „a state of complete physical, mental
and social well being”
WHO (1947)
Illness Cognitions 1 - qualitative
studies
Positive definitions
(energetic,
plenty of exercise, feeling fit, eating
the right things, being the correct
weight, having a good life / marriage)
Negative definitions
(don’t get
coughs and colds, only in bed once,
rarely go to the doctor and have
check-ups – nothing wrong)
Calnan (1987)
Physiological/physical
(e.g. good
condition, have energy)
Psychological
(e.g. happy, energetic)
Behavioural
(e.g. eat, sleep properly)
Future consequences
(e.g. live
longer)
The absence of…
(e.g. not sick, no
disease, no symptoms)
Lau (1995)
Lay people answered the question „what does it mean to be
healthy?”

What does it mean to be
sick?
Not feeling normal
(e.g. „I don’t feel right”)
Specific symptoms
(e.g. „physiological / psychological)
Specific illness
(e.g. cancer, cold, depression)
Consequences of illness
(e.g. how long the symptoms
last)
The absence of health
(e.g. not being healthy)
Lau (1995)

Illness Cognitions 3
„a patient’s own implicit common sense
beliefs about their illness”
(Leventhal et al.. 1980,
1997)
IC provide patients with a framework or a
scheme for:
–
coping with their illness
–
understanding their illness
–
telling them what to look out for if they are
becoming ill

Illness Cognitions 4
Five cognitive dimensions of these beliefs:
Identity
(label given to the illness and the symptoms experienced,
e.g. I have a cold <the diagnosis> with a runny nose <the symptoms>)
The perceived cause of the illness
(biological e.g. virus, or
psychosocial e.g. stress, smoking)
Time line
(how long the illness will last, whether it is short-term or
chronic)
Consequences
(physical e.g. pain, lack of mobility, emotional e.g.
loneliness, loss of social contact, a combination of factors, e.g. „My cold
will prevent me from playing football, which will prevent me from
seeing my friends”)
Curability and controllability
(e.g. „If I rest, my pain will go
away”, „If I get medicine from my doctor my cold will go away”)
(Leventhal et al.. 1980,
1997)

Illness Cognitions 5
Summing up:
Individuals may show consistant beliefs
about illness that can be used to make
sense of their illness and help their
understanding of any developing symptoms
(Ogden, 2000)
IC have been incorporated into a model of illness
behaviour to examine the relationship between an
individual’s cognitive representation of their illness
and their subsequent coping behaviour.
Why are IC’s important?
Stage 1:
Interpretation
• symptom perception
• social messages
- > Deviation from
norm
Representation
of health threat
•Identity
•Cause
•Consequences
•Time line
•Cure / control
Stage 2: COPING
• Approach coping
•Avoidance coping
Stage 3: Appraisal
• Was my coping
strategy effective?
Emotional
response to
health threat
•Fear
•Anxiety
•Depression
Leventhal’s self-regulatory model of illness
behaviour (Ogden J. (2000) Health
Psychology. A textbook. Buckingham: Open
University Press, s. 48)

Imagine you discover you have a strange
rush and increased temperature…
What do you think?
How do you feel?
What do you do?
Attitudes Towards Illness
(ATI) 1

Attitudes Towards Illness
(ATI) 2
The patients approach to the fact that
he/she has fallen ill and to the situation
of treatment and rehabilitation
Three components of ATI:
–
Cognitive
–
Affective
–
Motivational

ATI 3 – Cognitive Component
Information about causes and nature of the
illness, the principles of treatment and prevention
Ways of selecting, organizing and classifying
incoming information
Conceptualization of the self and future (family
life, career)
Expectations (towards medical staff, family
members etc)

ATI 4 – Affective Component
Emotions experienced with respect to the
illness, treatment and hospitalization
–
Anxiety
–
Fear
–
Hope
–
Anger
–
Harm/Loss etc
–
Denial

ATI 5 – Motivational
Component
Striving / determination
Intentions
Dispositions towards specific behaviour
related to illness and health

ATI 6 - modification
Cognitive
Component
„What is it?”
„What’s wrong with
me?”
„I feel just like my
Aunt Petunia – It
must be kidney
stone!”
Affective
Component
e.g. anxiety
Motivational
Component
„What can I do?”
„Shell I do
anything?”

ATI 7. Components – the
empirical indices
Cognitive component:
–
Range and adequacy of the patient’s
information concerning his/her illness, its
causes and treatment
–
Adequacy of the patient’s conceptualization
of his/her future professional capacities and
performance of family roles
–
Type of patient’s expectations concerning
the medical staff and family

ATI 8. Components – the
empirical indices
Affective component
–
Observation of the patients behaviour and
vegetative-somatic symptoms
–
voice, face expressions, topic he/she doesn’t want to
talk about
–
eyes!
Motivational component
–
How he/she behaves at the onset of symptoms and
during treatment and rehabilitation?
–
Plans for future?
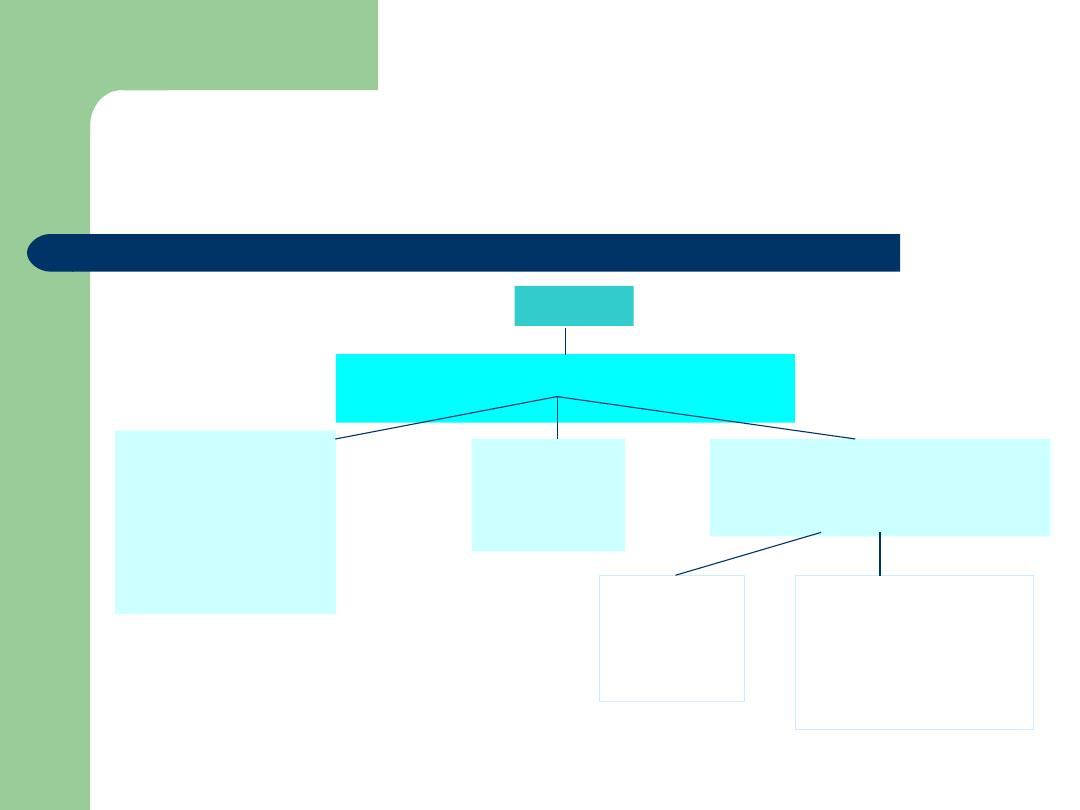
Attitudes Towards Illness 9
Disease
ATI (cognition+ emotions +
motivation)
Ambivalen
t attitude
(mixed)
Attitude
favourable for
the treatment
and
rehabilitation
process
Attitude unfavourable for
the course of treatment
and rehabilitation process
dominant
ANXIETY
compone
nt
dominant LACK
OF ACCEPTANCE
of the diagnosis
and medical
recommendations

OK, but what do I do to get to
know my patients true ATI or IC?
Questionnaire
Illness Perception Questionnaire (Weinman et al.. 1996)
ATI Questionnaire (Wrzesniewski) – polish version
Interview
Climate of security and understanding
Interview the patient in a skilled way
(and that’s what we’ll
practice soon)
LISTEN to the patient!
Remamber the 3 components of ATI and their empirical
indicies.

Case study
Determinants of the myocardial infarction (bio-
psycho-social risk factors).
The patient’s responses to illness and treatment
ATI components.
Implications for the doctor in charge of the case
and for the patients family.

Literature
This week reading:
–
Basic textbook, pages 39-52
–
Illness Perception Questionnaire at:
http://www.uib.no/ipq/
Reading for the next week:
–
Gorney, M., Bristow, J. (2003). Effective
physician communication skills. From:
http://www.thedoctors.com/risk/general/communication/J42
38.asp
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
Wyszukiwarka
Podobne podstrony:
TRANSIENT HYPOFRONTALITY AS A MECHANISM FOR THE PSYCHOLOGICAL EFFECTS OF EXERCISE
Effectiveness and side effects of anti CD20 therapy for autoantibody medicated blistering skin disea
The Effect of Childhood Sexual Abuse on Psychosexual Functioning During Adullthood
The Effects of Psychotherapy An Evaluation H J Eysenck (1957)
The effects of plant flavonoids on mammalian cells implication for inflammation, heart disease, and
Effect of long chain branching Nieznany
Effect of Kinesio taping on muscle strength in athletes
53 755 765 Effect of Microstructural Homogenity on Mechanical and Thermal Fat
Effect of File Sharing on Record Sales March2004
31 411 423 Effect of EAF and ESR Technologies on the Yield of Alloying Elements
21 269 287 Effect of Niobium and Vanadium as an Alloying Elements in Tool Steels
(10)Bactericidal Effect of Silver Nanoparticles
Effect of?renaline on survival in out of hospital?rdiac arrest
Effects of the Great?pression on the U S and the World
4 effects of honed cylinder art Nieznany
Effects of the Atomic Bombs Dropped on Japan
Some?finitions of Disease
Effect of aqueous extract
Effect of Active Muscle Forces Nieznany
więcej podobnych podstron