










FAST - Focused Assessment with Sonography for
Trauma
• FAST examines four areas for free
fluid:
– Perihepatic & hepato-renal space
– Perisplenic
– Pelvis
– Pericardium

The 4 FAST views

The 4 FAST views

Views for FAST U/S
• RUQ view is the most important view for FAST
• 80% of hemoperitoneum detected on
hepatorenal view alone
• If blood collects in the RUQ, the fluid settles
between the kidney and liver

Morrison’s Pouch

Liver
Morrison’s Pouch
Kidney

Normal Morrison’s pouch

Abnormal Morrison’s

LUQ view
• In this view, looking for blood between the
– Spleen and the kidney OR
– Spleen and the diaphragm

Abnormal LUQ

Pelvis view
• In this view, looking for blood in the
– Rectovesicular pouch (males)
– Rectouterine pouch aka pouch of Douglas (females)

Normal pelvis view

Abnormal pelvis view

Pericardial view
• In this view, looking for blood between the
pericardium and the heart

Normal pericardium

Abnormal pericardium

FAST vs DPL
FAST
DPL
Radiation
None
None
Rapid
++
+
Portable ++
+
Noninvasive Yes
No
Sensitive
Good
Excellent
Specificity
Good
Fair
Pericardial eval
Yes
No

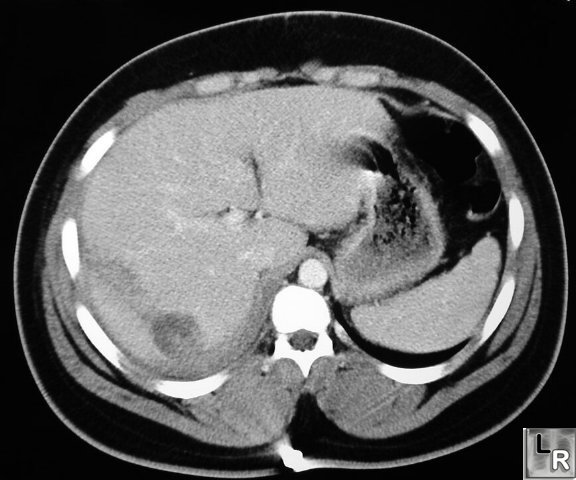
Contrast-enhanced CT of abdomen shows linear low-attenuation defectcrossing the
posterior aspect of the left lobe of the liver representing a laceration
Liver laceration

Liver laceration

Liver hematoma
Ultrasound examination shows the laceration as a
relatively hypoechoic area (arrow) with a local anechoic
area (arrowhead) that represents a haematoma

Liver hematoma

Spleen laceration

Spleen laceration and
hemoperitoneum

Kidney trauma
Axial contrast-enhanced CT section through
the kidneys showing extravasation of contrast
(arrow) from the left kidney, due to traumatic
forniceal rupture

Kidney trauma
Axial contrast-enhanced CT section shows a
large haematoma surrounding the fractured
lower pole of the right kidney.

Urinary bladder rupture
- requires prompt diagnosis so as to
avoid hyperkalemia, hypernatremia,
uremia, acidosis, and peritonitis;
- can be extraperitoneal or
intraperitoneal (or both);
- extraperitoneal
rupture:
- most often, the rupture is anterior and
extraperitoneal;
- in rare may result from laceration from
sharp bone spike;
- in many cases, may be treated non
operatively w/ suprapubic drainage;
- intraperitoneal rupture:
- occurs in about 15% of major pelvic
fractures;
- most often occurs from contussion to
lower abdomen or to the symphyseal
region;
- may occurs w/o associated pelvic ring
disruptions as the result of a seatbelt or
steering wheel injury;
- usually requires operative correction;
{kind=link}