
Leki w zaburzeniach
gospodarki wapniowej
dr hab. med. Ivan Kocić, prof.
nadzw. AMG

Calcium-Wapń
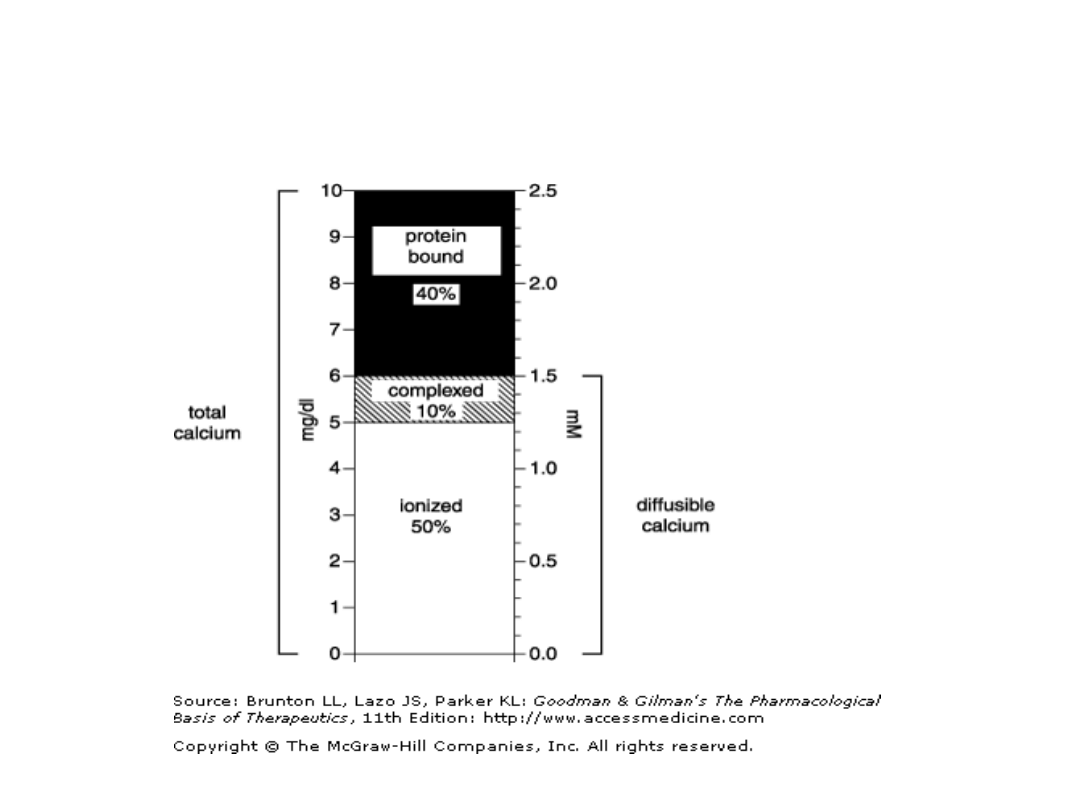
• Ca2+:
• Jony niezbędne do funkcji błon
biologicznych i
• skurczów mięśni,
• W płynie pozakomórkowym stężenie
mmol –istotne dla krzepnięcia krwi i
metabolizmu kości
Zasoby wapnia
CALCIUM
• Skeleton- 99% całkowitej
zawartości wapnia w
organizmie [Ca10(PO4)6(OH)2]
• + Na+, K+, Mg2+

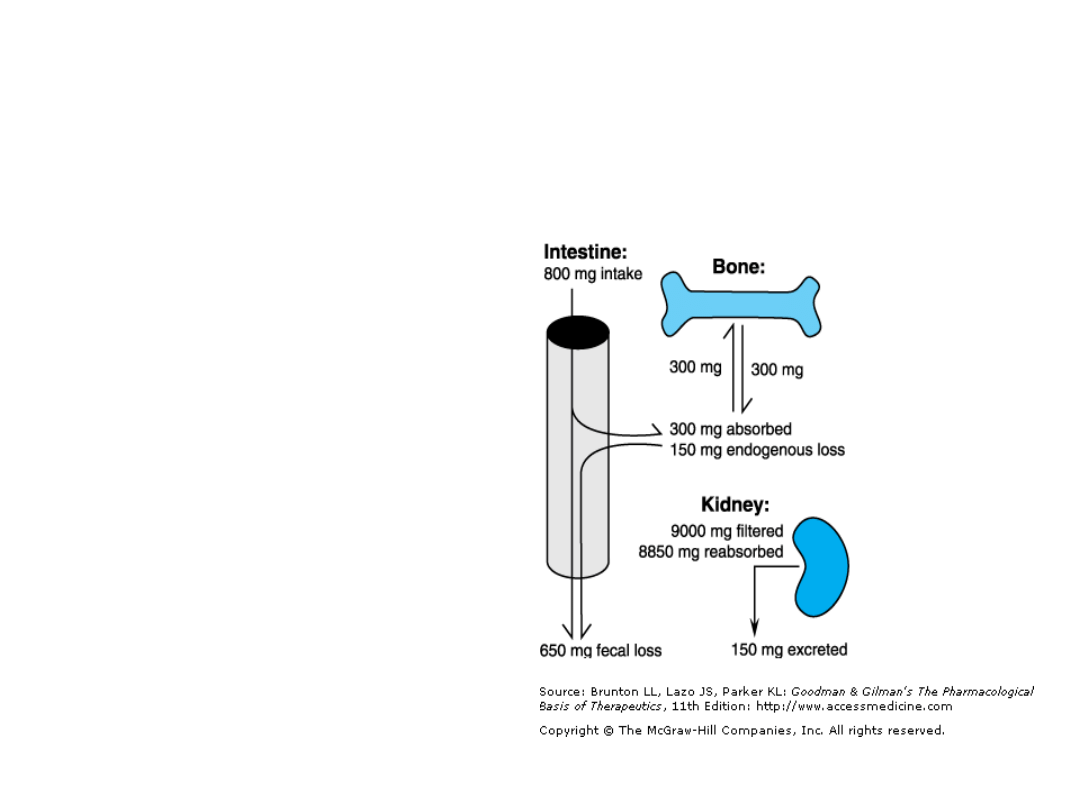
CALCIUM ABSORPTION AND
EXCRETION
• 75% z mleka i nabiału
• Odpowiednia norma to 1300 mg/d u młodzieży i
1000 mg/d u dorosłych
• Po 50 r. życia-1200 mg/d.
• Ca2+ wchodzi do organizmu przez jelita za
pomocą transportu aktywnego wymagajacego
obecność Vit. D (dwunastnica) i przez jelita
cienkie procesem ułatwionej dyfuzji-w większości.
Jednak, organizm również traci codziennie wapń
w ilości około 150 mg/d (żółć, śluz, stracone
komórki jelit)
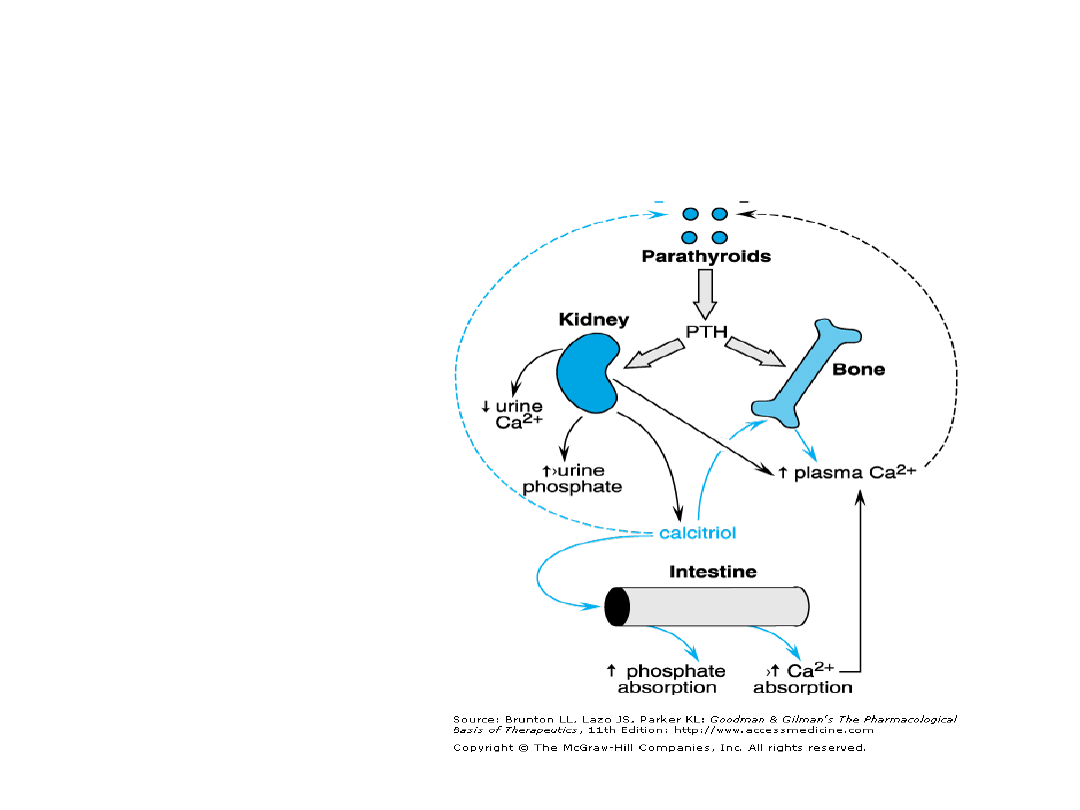
Regulacja metabolizmu wapnia
i fosforu
• PTH
• Vit D

Parathyroid Hormone (PTH)
• PTH-to hormon polipeptidowy,
regulujacy poziom jonów Ca2+ w
osoczu, poprzez wpływ na kości
(bone resorption/formation), Ca2+
eliminacje i wychwyt zwrotny w
nerkach i syntezę calcitriolu (Vit.D3)-
co zwieksza wchłanianie Ca2+ z
przewodu pokarmowego.

SYNTHESIS, SECRETION,
AND IMMUNOASSAY
• PTH is synthesized as a 115-amino-acid translation
product called preproparathyroid hormone. This
single-chain peptide is converted to
proparathyroid hormone by cleavage of 25 amino-
terminal residues as the peptide is transferred to
the intracisternal space of the endoplasmic
reticulum. Proparathyroid hormone then moves to
the Golgi complex, where it is converted to PTH by
cleavage of six amino acids. PTH(1–84) resides
within secretory granules until it is discharged into
the circulation. Neither preproparathyroid hormone
nor proparathyroid hormone appears in plasma.

PHYSIOLOGICAL
FUNCTIONS
• The primary function of PTH is to
maintain a constant concentration of
Ca2+ in the extracellular fluid. The
principal processes regulated are
renal Ca2+ absorption and
mobilization of bone Ca2+

Effects on Bone
• PTH increases bone resorption and thereby
increases Ca2+ delivery to the extracellular fluid.
This process involves the release of organic and
mineral matrix components (see below). The
apparent skeletal target cell for PTH is the
osteoblast, although evidence for the presence of
PTH receptors on mammalian osteoblasts is
limited. PTH also recruits osteoclast precursor cells
to form new bone remodeling units (see below).
• Direct effects of PTH on osteoblasts in vitro
generally are inhibitory and include reduced
formation of type I collagen, alkaline phosphatase,
and osteocalcin.

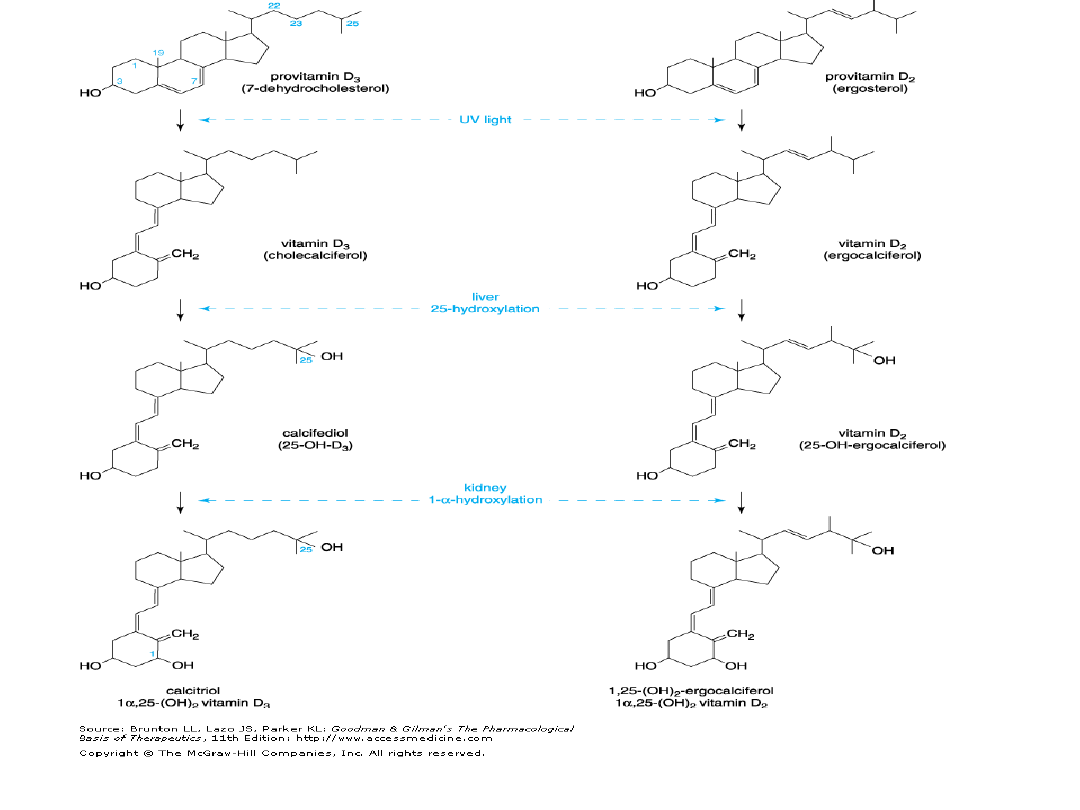
Vitamin D
• Vitamin D traditionally was viewed as a permissive
factor in calcium metabolism because it was thought
to permit efficient absorption of dietary calcium and
to allow full expression of the actions of PTH. We now
know that vitamin D exerts a more active role in
calcium homeostasis.
• Vitamin D is actually a hormone rather than a
vitamin; it is synthesized in mammals and, under
ideal conditions, probably is not required in the diet.
Receptors for the activated form of vitamin D are
expressed in many cells that are not involved in
calcium homeostasis, including hematopoietic cells,
lymphocytes, epidermal cells, pancreatic islets,
muscle, and neurons.

Wapń reguluje bardzo wiele
procesów zachodzących w
organizmie:
•
• Reguluje pH krwi ,co ma decydujący wpływ na nasze
zdrowie
• reguluje krzepliwość krwi, zmniejsza kruchość naczyń,
zwiększa ich przepuszczalność,
• zmniejsza reakcje alergiczne,
• niezbędne jest przy normalnej pracy mięśnia sercowego,
• kontroluje kurczenie i rozkurczanie mięśni,
• reguluje układ nerwowy, poprawiając przekazywanie
impulsów nerwowych,
• wspomaga działanie wielu bardzo ważnych enzymów,
• dobrze działa na płodność i donoszenie ciąży,
• pomaga w wyprowadzeniu z organizmu metali ciężkich,
• jest podstawowym składnikiem kości, zębów i paznokci,
wzmacnia włosy,
• zapobiega osteoporozie,
• obniża ciśnienie krwi,
• jest mocnym antyutleniaczem i antystreserem.
•

Niedobór wapnia objawia
się następującymi
symptomami
• zaburzeniami w rozwoju dziecka (późne ząbkowanie i
chodzenie, nadmierna potliwość, deformacje kości,
wczesna próchnica, nadmierna płaczliwość w nocy.
• skrzywieniem kręgosłupa i kończyn dolnych,
• skłonnością do alergii i wysypek,
• złą krzepliwością krwi (częste krwotoki, siniaki),
• skurczami mięśni i padaczką,
• bezsennością, zawrotami głowy, osłabieniem
pamięci, szybkim męczeniem się,
• bólami pleców, nóg, stawów oraz drętwieniem
kończyn,
• osteoporozą i skłonnością do złamań,
• częstymi zaparciami

HYPOCALCEMIA
• Mild hypocalcemia [i.e., reduction in ionized serum
Ca2+ concentrations from normal to concentrations
above 3.2 mg/dl (0.8 mM), approximately equal to a
total serum Ca2+ concentration of 8 to 8.5 mg/dl (2
to 2.1 mM)] is usually asymptomatic.
• The signs and symptoms of hypocalcemia include
tetany and related phenomena such as paresthesias,
increased neuromuscular excitability, laryngospasm,
muscle cramps, and tonic-clonic convulsions. In
chronic hypoparathyroidism, ectodermal changes—
consisting of loss of hair, grooved and brittle
fingernails, defects of dental enamel, and cataracts
—are encountered; calcification in the basal ganglia
may be seen on routine skull radiographs. Psychiatric
symptoms such as emotional lability, anxiety,
depression, and delusions often are present.
• Hypoparathyroidism is most often a
consequence of thyroid or neck surgery but
also may be due to genetic or autoimmune
disorders. In hypoparathyroidism,
hypocalcemia is accompanied by
hyperphosphatemia, reflecting decreased
PTH action on renal phosphate transport.
• Pseudohypoparathyroidism is a diverse
family of hypocalcemic and/or
hyperphosphatemic disorders.
Pseudohypoparathyroidism results from
resistance to PTH rather than PTH
deficiency; this resistance is not due to
mutations of the PTH receptor but rather to
mutations in Gs (GNAS1), which normally
mediates hormone-induced adenylyl
cyclase activation

• Neonatal tetany resulting from hypocalcemia
sometimes occurs in infants of mothers with
hyperparathyroidism; indeed, the tetany may
call attention to the mother's disorder.
• Hypocalcemia is associated with advanced
renal insufficiency accompanied by
hyperphosphatemia. Many patients with this
condition do not develop tetany unless the
accompanying acidosis is treated, which
decreases the ionized calcium. High
concentrations of phosphate in plasma inhibit
the conversion of 25-hydroxycholecalciferol
to 1,25-dihydroxycholecalciferol.
• Hypocalcemia also can occur following
massive transfusions with citrated blood,
which chelates calcium.
Preparaty wapnia

HYPERCALCEMIA
• Symptoms include fatigue, muscle
weakness, anorexia, depression, diffuse
abdominal pain, and constipation.
• Hypercalcemia can result from a number of
conditions. Ingestion of large quantities of
calcium by itself generally does not cause
hypercalcemia; exceptions are hyperthyroid
subjects, who absorb Ca2+ with increased
efficiency and subjects with the uncommon
milk-alkali syndrome, a condition caused by
concurrent ingestion of large quantities of
milk and absorbable alkali, resulting in
impaired renal Ca2+ excretion and
attendant hypercalcemia.

• Symptoms and signs of primary
hyperparathyroidism include fatigue,
exhaustion, weakness, polydipsia, polyuria,
joint pain, bone pain, constipation,
depression, anorexia, nausea, heartburn,
nephrolithiasis, and hematuria. This
condition frequently is accompanied by
significant hypophosphatemia owing to the
effects of PTH in diminishing renal tubular
phosphate reabsorption. Some patients
have renal calculi and peptic ulceration, and
a few display classical parathyroid skeletal
disease.

• Familial benign hypercalcemia (or familial
hypocalciuric hypercalcemia) is a genetic
disorder generally accompanied by extremely
low urinary calcium excretion. Hypercalcemia
usually is mild, and circulating PTH often is
normal to slightly elevated. The importance
of making this diagnosis lies in the fact that
patients mistakenly diagnosed as having
primary hyperparathyroidism may undergo
surgical exploration without discovery of an
adenoma and without therapeutic benefit.
• Diagnosis is established by demonstrating
hypercalcemia in first-degree family
members and a decreased fractional
excretion of calcium.

• Choroby nowotworowe:
Newly diagnosed hypercalcemia in
hospitalized patients is caused most often by a systemic
malignancy, either with or without bony metastasis. PTH-related
protein (PTHrP) is a primitive, highly conserved protein that may
be abnormally expressed in malignant tissue, particularly by
squamous cell and other epithelial cancers.
• Other tumors release cytokines or prostaglandins
that stimulate bone resorption. In some patients
with lymphomas, hypercalcemia results from
overproduction of 1,25-dihydroxyvitamin D by the
tumor cells owing to expression of 1 -hydroxylase.
A similar mechanism underlies the hypercalcemia
that is seen occasionally in sarcoidosis and other
granulomatous disorders.

• Nadmiar Vit.D może spowodować hypercalcemie jeżeli
wystarczająca iłość 25-hydroxyvitamin D jest obecna aby
spowodować zwiększony wychwyt Ca2+ z jelit
doprowadzając do hypercalcemii i zahamowaniu
wydzielania i obnizeniu poziomów PTH i 1,25-
dihydroxyvitamin D. Pomiar 25-hydroxyvitamin D jest
potrzebny do Dg.
• Pacjenci z hyperthyroidism mogą mieć umiarkowaną
hypercalcemie, chyba dzięki zwiększonej akcji kości
• Immobilization may lead to hypercalcemia in growing
children and young adults but rarely causes hypercalcemia
in older individuals unless bone turnover is already
increased, as in Paget's disease or hyperthyroidism.
• Hypercalcemia sometimes is noted in adrenocortical
deficiency, as in Addison's disease, or following removal of
a hyperfunctional adrenocortical tumor.
• Hypercalcemia occurs following renal transplantation owing
to persistent hyperfunctioning parathyroid tissue that
resulted from the previous renal failure.
• The differential diagnosis of hypercalcemia may pose
difficulties, but advances in serum assays for PTH, PTHrP,
and 25-hydroxy- and 1,25-dihydroxyvitamin D permit
accurate diagnosis in the great majority of cases.

Leki w leczeniu hiper-Ca2+
• Re hidratacja i wymuszona diureza
(furosemid): 500-1000ml/h
• Bisfosfonaty: Pamidronian 60-90mg jako wlew
i.v. przez 2-4h i zolendronian 4mg i.v. przez
15 min
• Kalcytonina 200 m.j. efekt po 4-6h i trwa 6-
10h
• Gallium Nitrate (leczenie nadmiaru wapnia u
chorych z nowotworami i choroba Pageta) :
200mg/m2 BSA/d w 5% dekstrozie przez 5 dni

• Plikamicyn (Mitramycin): 25-50 microg/kg
i.v. obniza istotnie poziom wapnia w
surowicy w trakcie 24-48h. Efekt utrzymuje
się przez kilka dni. Czasami występuje nagła
trombocytopenia
• Fosfaty: P, 1,5g w trakcie 6-8h: bardzo
pewna metoda obnizenia wapnia,ale
niebezpieczna, może doprowadzic do
gwałtownej hipocalcemii
• Sterydy: Przewlekła hipercalcemia w ramach
sarkoidozy, zatrucia Vit.D czy niektórych
nowotworów: prednizon 30-60 mg/per os
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
Wyszukiwarka
Podobne podstrony:
Patomechanizmy zaburzeń gospodarki wapniowo fosforanowej; osteoporoza
Choroby przytarczyc i zaburzenia gospodarki wapniowo fosforanowej
Wyklady kolo 2, Zaburzenia gospodarki wapniowo - fosforanowej
20. Zaburzenia gospodarki wapniowej, licencjat(1)
10 ZABURZENIA GOSPODARKI WAPNIOWO FOSFORANOWEJ
12 Patomechanizmy zaburzeń gospodarki wapniowo fosforanowej osteoporozaid 13289 ppt
Zaburzenia gospodarki wapniowo – fosforanowej, Rat med rok 2, Choroby wewnętrzne
Choroby przytarczyc i zaburzenia gospodarki wapniowo fosforanowej
FARMAKOLOGIA, 42 Leki w zaburzeniach gospodarki lipidowej
pediatria w[1] 9 zaburzenia gospodarki wapniowo fosforanowej u dzieci 16 04 08
Patomechanizmy zaburzeń gospodarki wapniowo fosforanowej; osteoporoza
Choroby przytarczyc i zaburzenia gospodarki wapniowo fosforanowej
Materiały Zaburzenia gospodarki wapniowo fosforanowej dla genetyków Taybert J
farmakologia 5 leki przeciwcukrzycowe i zaburz gosp wapniowej
I Leki regulujące zaburzenia gospodarki wodno elektrolitowej
W08 Patofizjologia zaburzeń gospodarki węglowodanowej
Diagnostyka laboratoryjna zaburzen gospodarki lek 2010
więcej podobnych podstron