Review
The role of child sexual abuse in the etiology
of suicide and non-suicidal self-injury
Maniglio R. The role of child sexual abuse in the etiology of suicide and
non-suicidal self-injury.
Objective: To address the best available scientific evidence on the role
of child sexual abuse in the etiology of suicide and non-suicidal self-
injury.
Method: Seven databases were searched, supplemented with hand-
search of reference lists from retrieved papers. The author and a
psychiatrist independently evaluated the eligibility of all studies
identified, abstracted data, and assessed study quality. Disagreements
were resolved by consensus.
Results: Four reviews, including about 65 851 subjects from 177
studies, were analyzed. There is evidence that child sexual abuse is a
statistically significant, although general and non-specific, risk factor
for suicide and non-suicidal self-injury. The relationship ranges from
small to medium in magnitude and is moderated by sample source and
size. Certain biological and psychosocial variables, such as serotonin
hypoactivity and genes, family dysfunction, other forms of
maltreatment, and some personality traits and psychiatric disorders,
may either act independently or interact with child sexual abuse to
promote suicide and non-suicidal self-injury in abuse victims, with
child sexual abuse conferring additional risk, either as a distal and
indirect cause or as a proximal and direct cause.
Conclusion: Child sexual abuse should be considered one of the several
risk factors for suicide and non-suicidal self-injury and included in
multifactorial etiological models.
R. Maniglio
Department of Pedagogic, Psychological, and Didactic
Sciences, University of Salento, Lecce, Italy
Key words: self-injury; suicide; child abuse; sexual
abuse; etiology; review
Roberto Maniglio, Department of Pedagogic, Psycho-
logical, and Didactic Sciences, University of Salento, Via
Stampacchia 45
⁄ 47, 73100 Lecce, Italy.
E-mail: robertomaniglio@virgilio.it
Accepted for publication September 7, 2010
Summations
• Child sexual abuse is a statistically significant, but modest, risk factor for suicidal and non-suicidal
self-injurious behaviour and ideation.
• Child sexual abuse may not have a primary role in the etiology of suicide and non-suicidal self-injury.
• Additional biological and psychosocial risk factors may, in some cases, be directly responsible for, or,
in other cases, contribute to the risk of suicidal and non-suicidal self-injurious behaviour by
mediating the relationship between child sexual abuse and self-injurious behaviour.
Considerations
• The role of child sexual abuse in the etiology of suicide and non-suicidal self-injury is complex.
• The presence of confounding variables and the poor quality of the studies do not allow for causal
inferences to be made.
• All studies included in this review did not assess data quality and validity and aggregated different
study findings, particularly those with different levels of methodological quality.
Acta Psychiatr Scand 2011: 124: 30–41
All rights reserved
DOI: 10.1111/j.1600-0447.2010.01612.x
2010 John Wiley & Sons A/S
ACTA PSYCHIATRICA
SCANDINAVICA
30

Introduction
Lethal and non-lethal self-inflicted injuries, includ-
ing completed and attempted suicide as well as non-
suicidal self-injury (i.e., intentional and direct self-
damaging acts causing bodily harm, without the
intent to die), are a serious public health problem
throughout the world (1–6) and present severe
repercussions on individuals, families, and society
at large (7), including direct and indirect economic
costs (8).
Given the seriousness of self-inflicted injuries,
much literature has attempted to investigate the
factors that promote suicidal and non-suicidal self-
injurious behaviours, with many clinicians and
researchers focusing on child sexual abuse as a
primary etiological factor. In fact, a growing
number of studies addressing the potential associ-
ation between sexual victimization in childhood
and suicide or non-suicidal self-injury in adoles-
cence or adulthood have been published over the
past 20 years. Efforts to summarize the findings of
these studies have resulted in several qualitative
and quantitative reviews.
It should be noted here that although extensive
evidence supports important distinctions between
suicidal and non-suicidal self-injurious behaviours
in terms of base rates, frequency, correlates,
lethality, and treatment outcomes (see 9), in the
literature on the sequelae of child abuse, suicidal
and non-suicidal forms of self-injury have been
often considered together as a common outcome
in survivors of child abuse (10, 11). For instance,
both
suicidal
behaviour
and
non-suicidal
self-injurious
behaviour
have
been
seen
as
deliberate self-damaging acts in which abuse
victims engage to reduce abuse-related distress
(see e.g., 12).
In general, literature reviews (e.g., 10, 11, 13–
35) have found high rates of suicidal and non-
suicidal self-injurious behaviours among victims
of child sexual abuse. However, there are funda-
mental questions concerning the nature and the
specific pathways of the association between child
sexual abuse and suicide and non-suicidal self-
injury that remain unanswered. Much of this
uncertainty might be attributable, in part, to the
methodological limitations of the literature on
child abuse. Most reviews of the empirical liter-
ature are characterized by imprecision and sub-
jectivity (see 31, 36). In fact, many reviews have
specified neither the data sources that were
searched nor the criteria used for including
studies. Furthermore, the majority of these liter-
ature reviews have not assessed data quality and
validity and have aggregated different study find-
ings, paying more attention to findings suggesting
harmful effects. As a result, causal inferences
cannot be made and conclusions cannot be drawn.
Thus, the role of sexual victimization in childhood
as a causal factor for suicide and non-suicidal self-
injury in adolescence or adulthood is not well
understood (11).
Aims of the study
To understand how and why some victims of early
sexual victimization self-injury in later life, this
paper provides a qualitative and semi-quantitative
analysis of the findings of the several reviews that
have addressed the literature on the association
between child sexual abuse and suicide and non-
suicidal self-injury. Given the severity of self-
inflicted injuries and with the current high levels
of public and scientific interest in child abuse, an
analysis of what is currently known about the
potential role of child sexual abuse in the etiology
of suicide and non-suicidal self-injury is required to
implement research and prevention efforts.
Material and methods
Given that this systematic review is part of a more
comprehensive review of the literature on child
sexual abuse, the methods are illustrated in detail
elsewhere (37, 38) and are only briefly described
here.
To obtain relevant studies, seven internet-based
databases (AMED, Cochrane Reviews, EBSCO,
ERIC, MEDLINE, PsycINFO, and ScienceDi-
rect) were searched for articles published between
January 1966 and December 2008. Separate
searches were conducted for the keywords child
(hood) sexual abuse and child(hood) sexual mal-
treatment. Further articles were identified by a
manual search of reference lists from retrieved
papers.
Studies were included whether they (i) appeared
in peer-reviewed journals; (ii) were published in
full; (iii) were critical reviews of the literature; (iv)
were not dissertation papers, editorials, letters,
conference proceedings, books, and book chapters;
(v) reviewed studies sampling human subjects; (vi)
investigated medical, neurobiological, psychologi-
cal, behavioural, sexual, or other health problems
following
childhood
sexual
abuse;
(vii)
had
primary and sufficient data derived from longitu-
dinal, cross-sectional, case–control, or cohort stud-
ies. For the purposes of the present systematic
review, only reviews that examined suicidal and
non-suicidal forms of self-injury following child
sexual abuse were included.
Child sexual abuse and self-injury
31
In accordance with guidelines for systematic
reviews (39–44), data were abstracted and study
quality was assessed on the basis of the following
criteria: (i) evidence identification, i.e., the data
sources (e.g., computerized databases, key jour-
nals, or reference lists from pertinent articles and
books) used to identify studies, including years
searched, keywords, and constraints; (ii) study
selection, i.e., the criteria used to select studies for
inclusion in the review; (iii) data extraction, i.e., the
process by which researchers obtained the neces-
sary information about study characteristics and
findings from the included studies; (iv) quality
assessment, i.e., the criteria or guidelines used for
assessing data quality and validity; (v) data syn-
thesis and analysis, i.e., the methods used to
analyze the results and the strength of evidence
as well as the description of the main results in an
objective, rigorous, and transparent fashion, with
the highest quality evidence available receiving the
greatest emphasis. Based on these criteria, each
study was assigned one of the following ratings:
good (study meets all criteria well), fair (study
does not meet one criterion), or poor (study does
not meet more than one criterion). Those studies
which were judged poor were rejected, because
they had important methodological limitations
that could invalidate their results.
Given that the assessment of all the papers by at
least two researchers working independently may
limit biases, minimize errors, improve reliability of
findings, reduce the possibility that relevant reports
will be discarded, and ensure that decisions and
judgments are reproducible (39, 41), the author,
R. M., and a psychiatrist, professor of Criminol-
ogy, independently evaluated the eligibility of all
studies identified, abstracted data, and assessed
study quality. Disagreements among authors were
discussed and resolved by consensus after review of
the article and the review protocol.
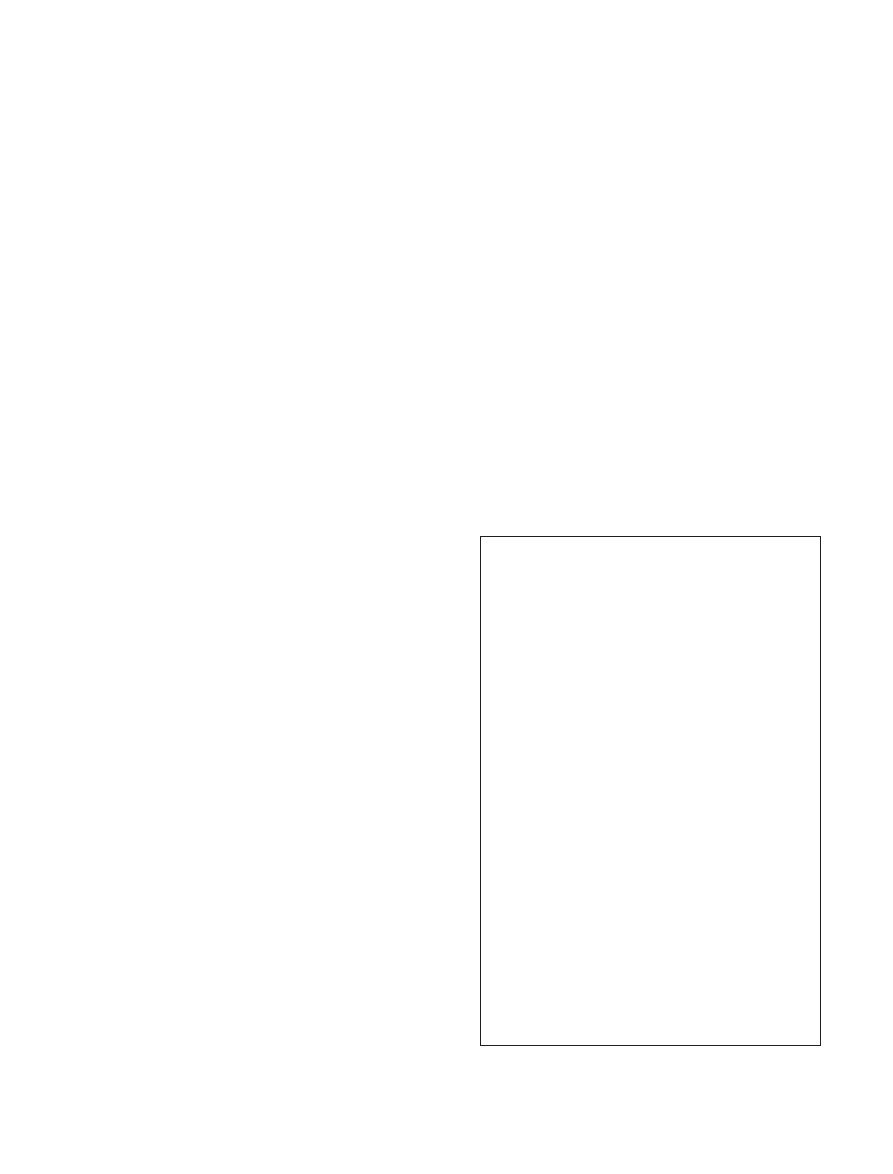
Results
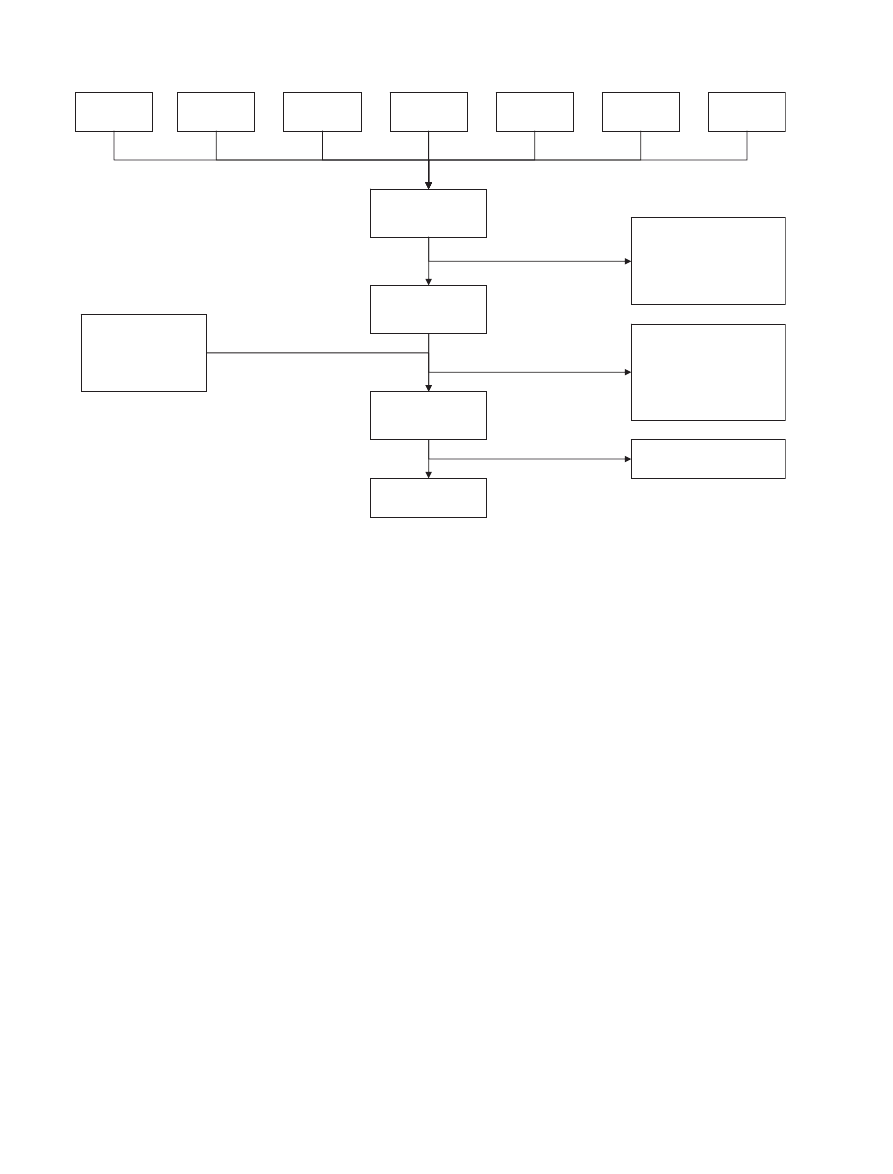
A total of 20 535 articles were identified. The
internet-based search identified 20 502 articles, 0
from AMED, 9 from Cochrane, 1550 from EBSCO,
1154 from ERIC, 2514 from MEDLINE, 7956 from
PsycINFO, and 7319 from ScienceDirect. Thirty-
three articles were identified by the manual search of
reference lists. Two hundred and forty-four full-text
articles were retrieved for more detailed evaluation
and 39 fulfilled all inclusion criteria. Of these, 35 did
not meet more than one of the quality criteria. For
these reasons, these studies were judged poor and
were rejected. Four reviews were judged fair,
because they did not meet the fourth criterion (i.e.,
they lacked a formal quality assessment) and were
included in this systematic review. A summary of
the study selection process is illustrated in Fig. 1.
Description of studies
The four reviews included in this systematic review
are described in Table 1. All the meta-analyses
were published between 1996 and 2008 and
reviewed a total of 177 studies (including 222
different subject samples, with 65 851 subjects). Six
(3.38%) of these studies were analyzed by more
than one review. The following sample types were
investigated: both young and adult subjects, only
adults, both males and females, and only females.
One of these meta-analyses focused on non-
suicidal self-injurious behaviour. All the other
reviews assessed suicide or non-suicidal self-injury
along with several other psychological or behavio-
ural sequelae of child sexual abuse. In the studies
included in each review, suicidal and non-suicidal
self-injurious behaviours were usually measured by
suicide and non-suicidal self-injury inventories,
scales, or questionnaires, investigator-authored
items or questions, or suicide and non-suicidal
self-injury-related items, or subscales from clinical
questionnaires, scales, and inventories.
All these reviews detailed the data sources used
to identify studies, the criteria used to select studies
for inclusion in the review, and the process by
which researchers acquired the necessary informa-
tion concerning study characteristics and findings
from the included studies. All the reviews under-
took a quantitative analysis of the data (i.e., meta-
analysis) to infer whether child sexual abuse was
significantly related to suicidal and non-suicidal
self-injurious behaviours and to estimate the
strength of this relationship. All the meta-analyses
described the main results in an objective fashion,
specified the methods that were employed to obtain
these results, took into account the strength of
evidence, investigated whether any observed effects
were consistent across studies, explored possible
reasons for any inconsistencies, and outlined how
heterogeneity was explored and quantified.
The following moderator variables were ana-
lyzed: form and date of publication of the study,
site of the study, size and source of the samples,
gender, socioeconomic status, and age of the
subjects at the time of assessment, sampling
strategy, method of assessment of abuse (e.g.,
questionnaire list), type of statistic used, definition
of child sexual abuse based on the maximum age of
victim, level of contact, consent, force, frequency,
and duration of abuse, relationship to the perpe-
trator (e.g., parent), age when abused. Multiple
Maniglio
32
regression, analysis of variance, and test of cate-
gorical models were used to determine whether
moderator variables accounted for significant
heterogeneity in effect sizes.
The main findings of the four meta-analyses
included in this systematic review are qualitatively
and semi-quantitatively analyzed in an evidence-
based, objective, and balanced fashion, with the
highest quality evidence available receiving the
greatest emphasis (45). To represent the degree of
the relationship between child sexual abuse and
suicide and non-suicidal self-injury, the effect size
estimators d and r were used. Positive d and r
values indicate higher levels of symptomatology for
sexually abused participants compared with con-
trol participants. According to Cohen (46), d of
0.20, 0.50, and 0.80, and r of 0.10, 0.30, and 0.50
correspond to small, medium, and large effect
sizes.
Strength of the association between child sexual abuse and
suicidal and non-suicidal self-injurious behaviour
In their review, Klonsky and Moyer (24) under-
took a meta-analysis of 45 samples from 43 studies,
with a total of 13 687 subjects, to address the
relationship between child sexual abuse and non-
suicidal self-injurious behaviour. Results showed
that child sexual abuse was significantly related to
non-suicidal self-injury. Such association was small
in magnitude.
Neuman et al. (26) provided 15 meta-analyses to
address the relationship of child sexual abuse with
a variety of psychological, behavioural, and sexual
problems, including self-mutilation and suicidal
ideation or behaviour. Three studies were used in
the non-suicidal self-injury meta-analysis and eight
in the suicidal ideation or behaviour meta-analysis.
Results indicated that child sexual abuse was
significantly related to suicidal and non-suicidal
self-injurious behaviour. The magnitudes of such
relationships were small to medium. Child sexual
abuse was significantly related also to all the other
problems, with magnitudes ranging from small to
medium.
In the review by Paolucci et al. (28), six meta-
analyses were undertaken to address the associa-
tion of child sexual abuse with a number of
psychological, behavioural, and sexual outcomes,
including suicidal ideation or behaviour. Ten
studies, with a total of 4008 subjects, were used
in the suicidal ideation or behaviour meta-analysis.
Results indicated a significant association between
child sexual abuse and suicidal ideation or behav-
iour. Such relationship was nearly medium in
magnitude. Child sexual abuse was significantly
AMED (n = 0)
Cochrane
(n = 9)
EBSCO
(n = 1550)
ERIC
(n = 1154)
Articles identified and
screened for retrieval
(n = 20 502)
Articles retrieved for
more detailed
evaluation (n = 211)
Articles excluded on title /
abstract review (n = 20 291):
editorials, letters, or conference
proceedings; no critical review
of the literature; no focus on
effects of child sexual abuse
Articles excluded on full-text
review (n = 205): no critical
review of the literature; no
focus on depression; no
sufficient data from
longitudinal, cross-sectional,
case-control, or cohort studies
Articles identified from
reference lists of
retrieved articles and
retrieved for detailed
evaluation (n = 33)
Articles included for
quality assessment
(n = 39)
MEDLINE
(n = 2514)
PsycINFO
(n = 7956)
Sciencedirect
(n = 7319)
Articles included
(n = 4)
Articles rejected on quality
assessment (n = 35)
Fig. 1.
Summary of study selection process.
Child sexual abuse and self-injury
33
Table
1.
Description
and
results
of
the
included
reviews
Source
Main
methods
Subjects
Outcome
variables
Moderator
variables
Significant
outcomes
(effect
sizes
or
odds
ratios
[95%
confidence
interval];
homogeneity)
Significant
moderators
(between-group
homogeneity)
Klonsky
&
Moyer
(24)
Systematic
search;
study
selection;
meta-analysis
Male
&
female
young
&
adult
patients
&
non-patients
(43
studies,
45
samples,
13
687
subjects)
Self-injurious
behaviour
Sample
size
and
source,
gender
and
age
of
the
subjects
at
the
time
of
assessment
Self-injurious
behaviour
(u
=
0.23
[0.20–0.26],
P
<
0.001;
Q
=
90.47,
P
<
0.001)
Sample
source
(Q
=
5.34,
P
<
0.001),
sample
size
(N
>
125:
u
=
0.21)
Neuman
et
al.
(26)
Systematic
search;
study
selection;
meta-analysis
Female
adult
patients
or
non-patients
(38
studies,
11
162
subjects)
Suicidal
ideation
or
behaviour
,
self-mutilation,
overall
psychopathology
,
anger
,
anxiety
,
depression,
revictimization,
sex
problems,
substance
abuse,
self-concept,
interpersonal
problems,
dissociation,
obsessions
or
compulsions,
somatization,
posttraumatic
stress,
general
symptoms
Publication
date
and
form,
sample
size
and
source,
age
of
subjects
at
the
time
of
assessment,
assessment
of
abuse,
type
of
statistic,
relationship
to
the
perpetrator
Suicidal
ideation
or
behaviour
(d
=
0.34
[0.24–0.44]),
self-mutilation
(d
=
0.42
[0.19–0.64]),
overall
psychopathology
(d
=
0.37
[0.33–0.41];
Q
=
62.36,
P
<
0.01),
anger
(d
=
0.39
[0.25–0.51]),
anxiety
(d
=
0.40
[0.34–0.47]),
depression
(d
=
0.41
[0.36–0.46]),
revictimization
(d
=
0.67
[0.50–0.84]),
sex
problems
(d
=
0.36
[0.30–0.42]),
substance
abuse
(d
=
0.41
[0.31–0.51]),
self-concept
(d
=
0.32
[0.32–0.47]),
interpersonal
problems
(d
=
0.39
[0.22–0.46]),
dissociation
(d
=
0.39
[0.32–0.47]),
obsessions
⁄
compulsions
(d
=
0.34
[0.22–0.46]),
somatization
(d
=
0.34
[0.24–0.45]),
posttraumatic
stress
(d
=
0.52
[0.44–0.59]),
general
symptoms
(d
=
0.46
[0.40–0.52])
Overall
impairment:
sample
source
(Q
B
=
9.40,
P
<
0.01)
Paolucci
et
al.
(28)
Systematic
search;
study
selection;
meta-analysis
Male
&
female
young
&
adult
patients
&
non-patients
(37
studies,
88
samples,
25
367
subjects)
Suicidal
ideation
or
behaviour
,
depression,
posttraumatic
stress,
early
sex
or
prostitution,
sex
perpetration,
intelligence
or
learning
Gender
and
socioeconomic
status
of
subjects
at
the
time
of
assessment,
level
of
contact
and
frequency
of
abuse,
relationship
to
the
perpetrator
,
age
when
abused
Suicidal
ideation
or
behaviour
(d
=
0.44
[0.40–0.48]),
depression
(d
=
0.44
[0.41–0.47]),
posttraumatic
stress
(d
=
0.40
[0.37–0.43]),
early
sex
⁄
prostitution
(d
=
0.29
[0.25–0.32]),
sex
perpetration
(d
=
0.16
[0.11–0.21]),
intelligence
⁄learning
(d
=
0.19
[0.12–0.26])
Maniglio
34
Table
1.
Continued
Source
Main
methods
Subjects
Outcome
variables
Moderator
variables
Significant
outcomes
(effect
sizes
or
odds
ratios
[95%
confidence
interval];
homogeneity)
Significant
moderators
(between-group
homogeneity)
Rind
et
al.
(31)
Systematic
search;
study
selection;
meta-analysis
Male
&
female
adult
non-patients
(59
studies,
51
samples,
15
635
subjects)
Suicidal
ideation
or
behaviour
,
overall
psychopathology
,
alcohol,
anxiety
,
depression,
dissociation,
eating
disorders,
hostility
,
interpersonal
sensitivity
,
locus
of
control,
obsessions
or
compulsions,
paranoia,
phobia,
psychosis,
self-esteem,
sex
problems,
social
impairment,
somatization,
general
symptoms
Publication
form,
study
site,
sampling
strategy
,
gender
and
age
of
the
subjects
at
the
time
of
assessment,
sampling
strategy
,
assessment
of
abuse,
age
of
victim
in
abuse
definition,
level
of
contact,
consent,
force,
frequency
,
and
duration
of
abuse,
relationship
to
the
perpetrator
Suicidal
ideation
or
behaviour
(r
=
0.09
[0.06–0.12];
v
2
=
10.94),
overall
psychopathology
(r
=
0.09
[0.08–0.11];
v
2
=
49.19,
P
>
0.50),
alcohol
(r
=
0.07
[0.02–0.12];
v
2
=
2.97),
anxiety
(r
=
0.13
[0.10–0.15];
v
2
=
4.62),
depression
(r
=
0.12
[0.10–0.14];
v
2
=
25.71),
dissociation
(r
=
0.09
[0.04–0.15];
v
2
=
1.86),
eating
disorders
(r
=
0.06
[0.02–0.10];
v
2
=
9.92),
hostility
(r
=
0.11
[0.06–0.16];
v
2
=
11.22,
P
<
0.05),
interpersonal
sensitivity
(r
=
0.10
[0.06–0.15];
v
2
=
11.78),
obsessions
⁄
compulsions
(r
=
0.10
[0.06–0.15];
v
2
=
5.01),
paranoia
(r
=
0.11
[0.07–0.16];
v
2
=
10.34),
phobia
(r
=
0.12
[0.07–0.17];
v
2
=
8.08),
psychosis
(r
=
0.11
[0.06–0.15];
v
2
=
10.13),
self-esteem
(r
=
0.04
[0.01–0.07];
v
2
=
51.31,
P
<
0.05),
sex
problems
(r
=
0.09
[0.07–0.11];
v
2
=
39.49,
P
<
0.05),
social
impairment
(r
=
0.07
[0.04–0.10];
v
2
=
20.37),
somatization
(r
=
0.09
[0.06–0.12];
v
2
=
15.20),
general
symptoms
(r
=
0.12
[0.08–0.15];
v
2
=
18.77)
Overall
impairment:
incest
(r
=
0.09),
gender
⁄consent
interaction
(z
=
2.51,
P
>
0.02;
females,
r
=
0.11
[0.09–0.13];
v
2
=
14.50)
Child sexual abuse and self-injury
35
related also to all the other outcomes, with
magnitudes ranging from small to medium.
Rind et al. (31) provided 18 meta-analyses to
address the relationship of child sexual abuse with
a variety of psychological, behavioural, and sexual
problems, including suicidal ideation or behaviour.
Nine samples, with a total of 5425 subjects,
were used in the suicidal ideation or behaviour
meta-analysis. Results showed that child sexual
abuse was significantly related to suicidal ideation
or behaviour. The magnitude of such relationship
was of small size. Child sexual abuse was signifi-
cantly related to several other outcomes, with
magnitudes of small size.
Moderators of the relationship between child sexual abuse and
suicidal and non-suicidal self-injurious behaviour
Klonsky and Moyer (24) found that the distribu-
tion of effect size estimates exhibited significant
heterogeneity. An analog of an analysis of variance
procedure appropriate for effect size data showed
that sample type was a significant moderator of the
relationship between abuse and non-suicidal self-
injury. This relationship was stronger for the
clinical samples than for the non-clinical samples.
Further analysis of effect sizes revealed that some
explanation of effect size variance was also
accounted for by sample size. Studies with larger
samples (N > 125) reported smaller effect sizes.
According to the authors, this result suggested the
possibility of a bias toward publishing studies with
statistically significant results, because studies with
smaller sample sizes required larger effect sizes to
achieve statistical significance. Indeed, formal
analyses found evidence of publication bias, sug-
gesting that smaller studies with positive findings
were more likely to be published than smaller
studies with null or negative findings.
In the review by Neuman et al. (26), a significant
heterogeneity among effect sizes was found. Focus-
ing on the sample-level rather than symptom-level
effect sizes, the authors found that the variability in
sample-level effect sizes could be accounted for by
sample source. Clinical samples generated larger
effect sizes. There was a tendency for studies with
smaller samples (N < 50) to yield comparatively
high mean effect sizes, compared to studies that
examined larger numbers of subjects.
In the review by Paolucci et al. (28), a series of
analyses of variance revealed that none of the
moderators was statistically significant.
Rind et al. (31) found that the effect sizes were
generally homogeneous. Further analysis of the
sample-level effect sizes indicated that larger effect
size estimates were significantly linked to intra-
familial abuse and definition of abuse including
both willing and unwanted sex (only for women).
Importantly, certain family variables (i.e., physical
or emotional abuse and neglect, adaptability, con-
flict or pathology, family structure, support or
bonding, and traditionalism) were confounded with
child sexual abuse. The confounding of child sexual
abuse and family environment raised the possibility
that child sexual abuse was not causally related to
outcomes or was related in a smaller way than
uncontrolled analyses had indicated. To address
this issue, the relationship between family variables
and symptoms was examined. Thus, 18 further
meta-analyses were provided. Two samples, includ-
ing 634 subjects, were used in the suicidal ideation
or behaviour meta-analysis. Results showed that
family environment was significantly related to
suicidal ideation or behaviour (r = 0.26; 95%
confidence interval: [
)0.18 to 0.33]). The magnitude
of such relationship was medium to large, and, thus,
larger than that of the association between child
sexual abuse and suicidal ideation or behaviour.
Discussion
Main results from the studies
i) Across methodologies, samples, and mea-
sures, there is a statistically significant
association between child sexual abuse and
suicidal
and
non-suicidal
self-injurious
behaviour or ideation.
ii) The magnitude of the relationship between
child sexual abuse and suicide and non-
suicidal self-injury ranges from small to
medium.
iii) Child sexual abuse is significantly related
also to several other psychological and
behavioural problems.
iv) Sample source and sample size account, in
part, for effect size variance, with studies
with smaller samples and subject samples
drawn from clinical populations reporting
larger effect sizes.
v) All the other moderators generate conflicting
or non-significant results: more severe and
traumatic forms of sexual victimization such
as those involving force, violence, penetra-
tion, longer duration, and high frequency of
sexual contact do not increase the likelihood
of suicide and non-suicidal self-injury in
people who have been sexually victimized
as children.
The results of the four meta-analyses included
in
this
systematic
review
show
that
across
Maniglio
36

methodologies, samples, and measures, survivors
of child sexual abuse are significantly at risk of
suicide and non-suicidal self-injury. However, child
sexual abuse was significantly related also to
several other psychological and behavioural prob-
lems. Therefore, child sexual abuse should be
considered a general, non-specific risk factor for
suicidal and non-suicidal self-injurious behaviours.
The magnitude of the relationship between child
sexual abuse and suicide and non-suicidal self-
injury ranged from small to medium. Moderator
analyses revealed that sample source and sample
size accounted, in part, for effect size variance.
More specifically, studies with smaller samples
reported larger effect sizes. This result suggests the
possibility of publication bias, with smaller studies
with positive findings being more likely to be
published than smaller studies with null or negative
findings (24). Furthermore, subject samples drawn
from clinical populations yielded larger effect sizes
than did subject samples drawn from non-clinical
samples. This result suggests that psychiatric sam-
ples tend to exclude well-adjusted survivors of
sexual abuse because these samples are likely to
constitute the negative extreme of abuse outcomes
(31). In contrast, community and student samples
tend to include more well-adjusted abuse survivors,
because a certain level of wellness is required to
perform daily activities, such as occupational tasks,
school
obligations,
family
responsibilities,
or
household activities.
All the other moderators generated conflicting or
non-significant
results.
Many
clinicians
and
researchers (see, e.g., 11, 14, 15) have suggested
that the relationship between child sexual abuse
and suicide and non-suicidal self-injury may be
greater for more severe and traumatic forms of
sexual victimization, such as those involving force,
violence, penetration, longer duration, and high
frequency of sexual contact. Nevertheless, the
results of this systematic review do not confirm
suspicions that such factors concerning aspects of
the abuse experience increase the likelihood of
suicide and non-suicidal self-injury in people who
have been sexually victimized as children.
Causality issues
The results of this systematic review show a
statistically significant, but modest association
between child sexual abuse and suicidal and non-
suicidal self-injurious behaviours. However, it
should be noted that causal inferences cannot be
made, because of the presence of confounding
variables and methodological weaknesses in the
studies included in each review. Many of the
studies investigating the relationship between
child abuse and suicide or non-suicidal self-injury
are characterized by a generally poor methodolog-
ical quality (14). Indeed, most studies have design,
sampling, and measurement problems, such as
poor sampling methods, absence of appropriate
comparison groups, inadequate operationalization
and measurement of abuse histories and outcomes,
insufficient control for effect modifiers and con-
founders, or designs inappropriate to prove cau-
sality. In addition, it should be noted that all the
reviews included in this systematic review did not
assess data quality and validity and aggregated
different study findings, particularly those with
different levels of methodological quality. There-
fore, findings should be interpreted cautiously.
Most importantly, much of the traditional
empirical research on the relationship between
child sexual abuse and suicide or non-suicidal self-
injury has not controlled for the overlap with other
biological, psychological, or social factors that
increase the risk of suicidal and non-suicidal self-
injurious behaviours (see e.g., 11). Thus, it is
unclear whether suicide and non-suicidal self-
injury in subjects who have been sexually abused
in childhood may be attributable to early sexual
abuse or whether suicidal and non-suicidal self-
injurious behaviours may be attributable to other
risk factors that may precede, accompany, or
follow the experience of child sexual abuse.
Several reviews have shown that suicide and
non-suicidal self-injury are related to genetic com-
ponents (47–56), abnormalities in the serotonergic
system (57–60), other forms of child abuse, espe-
cially emotional (61) and physical maltreatment
(21, 62, 63), dysfunctional family relationships and
climate, especially impaired or unsatisfying parent–
adolescent relationships, unsupportive parenting,
high family conflict, low family cohesion, parental
divorce, and ineffective family communication (20,
21, 34, 64), personality variables, especially aggres-
sion (21, 32, 65–67), impulsivity (21, 32, 67),
hopelessness (20, 21, 32, 65, 68, 69), negative
affectivity (see 70), and ineffective problem-solving
ability (21, 32), and psychiatric disorders (20, 21,
65), especially schizophrenia (71, 72) depressive
(73–76), personality (77; see also 78), and sub-
stance-related disorders (79–82), anorexia nervosa
(83, 84), and bipolar (76, 85-87; see also 88),
attention deficit hyperactivity (89), and posttrau-
matic stress disorder (90).
Some of these factors might better account for
the risk of self-injury and suicide in people who
have been sexually victimized as children, rather
than the experience of child sexual abuse itself
having a causal role in the etiology of suicide and
Child sexual abuse and self-injury
37

non-suicidal self-injury. More specifically, there is
evidence that the various forms of child maltreat-
ment are highly prevalent and intercorrelated in
dysfunctional families (13, 63, 91, 92). Speaking
more broadly, it has been noted that, in these
distressed families, it is difficult to determine the
specific effects of child sexual abuse over and above
the effects of dysfunctional environment and
genetic contribution (14, 63, 91, 93), because of
the high prevalence of family problems and co-
occurring forms of child maltreatment as well as
histories of substance abuse, psychiatric disorders,
and suicidal behaviour among parents that may be
transmitted to their offspring (93). For example, in
the meta-analysis by Klonsky and Moyer (24),
those studies that controlled for borderline per-
sonality disorder and family environment revealed
a minimal or negligible relationship between child
sexual abuse and non-suicidal self-injury. In the
meta-analysis by Rind et al. (31), certain family
variables (e.g., family structure, conflict, pathol-
ogy, support or bonding, and traditionalism) were
confounded with child sexual abuse and more
strongly related to suicidal ideation and behaviour
than was child sexual abuse.
In sum, it is possible that, in abusive contexts or
dysfunctional families, both environmental and
biological factors may increase the risk of suicidal
and non-suicidal self-injurious behaviours in off-
spring (93). Multiple risk factors for suicide and
non-suicidal self-injury other than child sexual
abuse, such as a family history of suicidal behav-
iour, mental illness, or substance abuse in parents
and offspring, family conflict or dysfunction, and
other forms of child abuse, might also be present in
these dysfunctional contexts. Some of these factors
may be directly responsible for suicide and non-
suicidal self-injury in the survivors of child sexual
abuse.
In addition, other factors may contribute to the
likelihood of suicidal and non-suicidal self-injuri-
ous behaviours in adolescent or adults who were
sexually abused as children by mediating the
relationship between early sexual victimization
and self-injurious behaviour. In fact, it is possible
that the effects of child sexual abuse on later
suicide and non-suicidal self-injury may operate
through the mediating influences of other vari-
ables, such as neurobiological substrates and
certain personality traits or psychiatric disorders.
In other words, it is possible that child sexual abuse
may promote other biological or psychological
conditions which, in turn, might lead the victim to
engage in suicide and non-suicidal self-injury. In
these cases, child sexual abuse would not have a
direct pathway to suicidal and non-suicidal self-
injurious behaviours but instead would have a
direct relationship with another condition, which,
in turn, would have a direct pathway to self-
injurious behaviour.
More specifically, it is possible that child sexual
abuse may influence suicidal and non-suicidal
self-injurious behaviour by negatively affecting
neurobiological or personality development. For
example, it has been hypothesized that sexual
abuse in childhood may set serotonergic function
at a lower level (94). This effect might persist into
adolescence or adulthood, contributing to the
increased risk for suicidal and non-suicidal self-
injurious behaviours. It has been also suggested
that the effects of serotonin hypoactivity and genes
on suicidal behaviour may operate through impul-
sivity and aggression (32, 65). Furthermore, in the
meta-analysis by Klonsky and Moyer (24), those
studies that controlled for hopelessness suggested
that the relationship between child sexual abuse
and non-suicidal self-injury became minimal or
negligible. Therefore, it is possible that the rela-
tionship between child sexual abuse and suicidal
and non-suicidal self-injurious behaviour might be
mediated by neurobiological alterations and some
personality variables, such as impulsivity (95),
aggression (95), poor problem-solving skills (35),
and hopelessness (35).
Most importantly, in many cases, psychological
disturbance, in terms of dysfunctional personality
traits or psychiatric disorders following child
abuse, may lead child sexual abuse survivors to
self-injury to reduce painful abuse-related internal
states. A literature review has shown that most
non-suicidal self-injurers identify the desire to
alleviate negative affect as a reason for self-
injuring and present decreased negative affect
and relief after self-injury (96). It has been
hypothesized that suicidal and non-suicidal self-
injurious behaviours may be seen as emotionally
avoidant coping activities, i.e., behavioural strat-
egies employed to temporarily avoid, reduce,
anesthetize, interrupt, or alleviate unpleasant
internal states, such as, thoughts, memories, feel-
ings, or affects, associated with an abuse history,
to provide survivors with a temporary sense of
calm and relief, at least for some period of time
(10, 12, 16–18, 29, 32, 95–99). In other words, it is
possible that child sexual abuse might lead to
psychic distress, in terms of dysfunctional person-
ality traits, psychiatric disorders, or painful abuse-
related internal states, which, in turn, might lead
child abuse victims to employ emotionally avoi-
dant coping behaviours, such as self-inflicted
injuries, to achieve temporary relief, especially
when these individuals also have concurrent prob-
Maniglio
38

lem-solving deficiencies or poor coping skills (100,
101). Although often effective in the short term,
emotionally avoidant coping strategies are rarely
adaptive in the long term, leading to repeated
cycles of self-inflicted injuries in the presence of
future pain, subsequent calm, the slow building of
further tension, and, ultimately, further self-harm
(16).
In conclusion, the results of this systematic review
reveal that the role of child sexual abuse in the
etiology of suicide and non-suicidal self-injury is
complex. Being a victim of child sexual abuse is a
significant, although general and non-specific, risk
factor for suicidal and non-suicidal self-injurious
behaviour and ideation. However, child sexual abuse
is not the only important risk factor for suicide and
non-suicidal self-injury. Evidence to date suggests
that, in many cases, child sexual abuse has not a
primary role in the etiology of suicidal and non-
suicidal self-injurious behaviour. Additional biolog-
ical, psychological, and social risk factors, such as
serotonin hypoactivity and genes, family dysfunc-
tion, co-occurring forms of child maltreatment, and
certain personality traits and psychiatric disorders
may, in some cases, be directly responsible for suicide
and non-suicidal self-injury, or, in other cases,
contribute to the risk of self-inflicted injuries by
mediating the relationship between child sexual abuse
and suicide and non-suicidal self-injury. However, it
is apparent that being a victim of child sexual abuse
may sometimes confer additional risk of suicidal and
non-suicidal self-injurious behaviour either as a
distal and indirect cause or as a proximal and
direct cause. Thus, child sexual abuse should be
considered one of the several risk factors for suicide
and non-suicidal self-injury and included in multi-
factorial etiological models to elucidate the mecha-
nisms that contribute to self-injury in survivors of
child abuse. To achieve this goal, several methodo-
logical advances in research in this area are required,
such as use of longitudinal designs, control for
confounders, employment of study samples repre-
sentative of the general population and matched
comparison groups, and, for literature reviews,
assessment of data quality and validity.
Acknowledgement
I thank Oronzo Greco, MD, University of Salento, Lecce,
Italy, for his help on study selection, data abstraction, and
quality assessment.
Declaration of interest
This study has no external funding source and was not
financial supported. The author has indicated he has no
financial relationships relevant to this article to disclose. The
author has not other interests in specific in relation to the
pharma industry without any direct connection to this study.
References
1. Bertolote JM, Fleischmann A. Suicidal behavior preven-
tion: WHO perspectives on research. Am J Med Genet
2005;133:8–12.
2. Levi F, La Vecchia C, Lucchini F et al. Trends in mortality
from
suicide,
1965–99.
Acta
Psychiatr
Scand
2003;108:341–349.
3. Moscicki EK. Epidemiology of completed and attempted
suicide: toward a framework for prevention. Clin Neu-
rosci Res 2001;1:310–323.
4. Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee
S
.
Suicide
and
suicidal
behavior.
Epidemiol
Rev
2008;30:133–154.
5. World Health Organization. Prevention of suicide:
guidelines for the formulation and implementation of
national strategies. Geneva: World Health Organization,
1996.
6. World Health Organization. The global burden of dis-
ease: 2004 update. Geneva: World Health Organization,
2008.
7. Miller TR, Covington K, Jensen A. Costs of injury by
major cause, United States, 1995: cobbling together esti-
mates. In: Mulder S, Van Beeck EF, eds. Measuring the
burden of injury. Amsterdam: ECOSA, 1999:23–40.
8. Goldsmith SK, Pellmar TC, Kleinman AM et al. Reducing
suicide: a national imperative. Washington, DC: National
Academies Press, 2002.
9. Nock MK ed. Understanding non-suicidal self-injury:
origins, assessment, and treatment. Washington, DC:
American Psychological Association, 2009.
10. Yates TM. The developmental psychopathology of
self-injurious
behavior:
compensatory
regulation
in
posttraumatic adaptation. Clin Psychol Rev 2004;24:
35–74.
11. Santa Mina EE, Gallop RM. Childhood sexual and phys-
ical abuse and adult self-harm and suicidal behaviour: a
literature review. Can J Psychiatry 1998;43:793–800.
12. Briere J. Child abuse trauma: theory and treatment of the
lasting effects. Newbury Park, CA: Sage, 1992.
13. Bagley C. The long-term psychological effects of child
sexual abuse: a review of some British and Canadian studies
of victims and their families. Ann Sex Res 1991;4:23–48.
14. Beitchman JH, Zucker KJ, Hood JE, Dacosta GA, Akman D.
A review of the short-term effects of child sexual abuse.
Child Abuse Negl 1991;15:537–556.
15. Beitchman JH, Zucker KJ, Hood JE, Dacosta GA, Akman D,
Cassavia
E
. A review of the long-term effects of child
sexual abuse. Child Abuse Negl 1992;16:101–118.
16. Briere JN, Elliot DM. Immediate and long term impacts
of child sexual abuse. Future Child 1994;4:54–69.
17. Briere JN, Runtz M. Childhood sexual abuse: long-term
sequelae and implications for psychological assessment.
J Interpers Violence 1993;8:312–330.
18. Briere J, Runtz M. The long-term effects of sexual
abuse: a review and synthesis. New Dir Ment Health
Serv 1991;51:3–13.
19. Browne A, Finkelhor D. Impact of child sexual abuse:
a review of the research. Psychol Bull 1986;99:66–77.
20. Evans E, Hawton K, Rodham K. Factors associated with
suicidal phenomena in adolescents: a systematic review of
Child sexual abuse and self-injury
39
population-based studies. Clin Psychol Rev 2004;24:957–
979.
21. Gould MS, Greenberg T, Velting D, Shaffer D. Youth
suicide risk and preventive interventions: a review of the
past 10 years. J Am Acad Child Adolesc Psychiatry
2003;42:386–405.
22. Holmes WC, Slap GB. Sexual abuse of boys: definition,
prevalence, correlates, sequelae, and management. JAMA
1998;280:1855–1862.
23. Kendall-Tackett K, Williams LM, Finkelhor D. Impact of
sexual abuse on children: a review and synthesis of recent
empirical studies. Psychol Bull 1993;113:164–180.
24. Klonsky ED, Moyer A. Childhood sexual abuse and non-
suicidal
self-injury:
meta-analysis.
Br
J
Psychiatry
2008;192:166–170.
25. Mulvihill D. The health impact of childhood trauma: an
interdisciplinary review, 1997–2003. Issues Compr Pediatr
Nurs 2005;28:115–136.
26. Neumann DA, Houskamp BM, Pollock VE, Briere J. The
long-term sequelae of childhood sexual abuse in women:
a meta-analytic review. Child Maltreat 1996;1:6–16.
27. Nurcombe B. Child sexual abuse I: psychopathology. Aust
N Z J Psychiatry 2000;34:85–91.
28. Paolucci EO, Genuis ML, Violato C. A meta-analysis of
the published research on the effects of child sexual abuse.
J Psychol 2001;135:17–36.
29. Polusny MA, Follette VM. Long-term correlates of child
sexual abuse: theory and review of the empirical litera-
ture. Appl Prev Psychol 1995;4:143–166.
30. Putnam F. Ten year research update review: child sexual
abuse. J Am Acad Child Adolesc Psychiatry 2003;42:269–
278.
31. Rind B, Tromovitch P, Bauserman R. A meta-analytic
examination of assumed properties of child sexual abuse
using college samples. Psychol Bull 1998;124:22–53.
32. Spirito A, Esposito-Smythers C. Attempted and completed
suicide
in
adolescence.
Annu
Rev
Clin
Psychol
2006;2:237–266.
33. Valente SM. Sexual abuse of boys. J Child Adolesc Psy-
chiatr Nurs 2005;18:10–16.
34. Wagner BM. Family risk factors for child and adolescent
suicidal behavior. Psychol Bull 1997;121:246–298.
35. Yang B, Clum GA. Effects of early negative life experi-
ences on cognitive functioning and risk for suicide:
a review. Clin Psychol Rev 1996;16:177–195.
36. Rind B, Tromovitch P. A meta-analytic review of findings
from national samples on psychological correlates of
child sexual abuse. J Sex Res 1997;34:237–255.
37. Maniglio R. The impact of child sexual abuse on health: a
systematic
review
of
reviews.
Clin
Psychol
Rev
2009;29:647–657.
38. Maniglio R. Child sexual abuse in the etiology of
depression: a systematic review of reviews. Depress
Anxiety 2010;27:631–642.
39. Centre for Reviews and Dissemination. CRDs guidance
for undertaking reviews in health care. York: University
of York Press, 2008.
40. Egger M, Davey Smith G, Altman DG. Systematic reviews
in health care: meta-analysis in context, 2nd edn. London:
BMJ Publication Group, 2001.
41. Higgins JPT, Green S. Cochrane handbook for systematic
reviews of interventions. Chichester: John Wiley & Sons,
2006.
42. Lipsey MW, Wilson DB. Practical meta-analysis. Thou-
sand Oaks, CA: Sage, 2000.
43. Petticrew M, Roberts H. Systematic reviews in the social
sciences: a practical guide. Malden, MA: Blackwell Pub-
lishing, 2006.
44. Stroup DF, Berlin JA, Morton SC et al. Meta-analysis of
observational studies in epidemiology: a proposal for
reporting. JAMA 2000;283:2008–2012.
45. Slavin RE. Best evidence synthesis: an intelligent alter-
native to meta-analysis. J Clin Epidemiol 1995;48:9–18.
46. Cohen J. Statistical power analyses for the behavioral
sciences, 2nd edn. Hillsdale, NJ: Erlbaum, 1988.
47. Anguelova M, Benkelfat C, Turecki G. A systematic re-
view of association studies investigating genes coding for
serotonin receptors and the serotonin transporter: II.
Suicidal behavior. Mol Psychiatry 2003;8:646–653.
48. Arango V, Huang YY, Underwood MD, Mann JJ. Genetics
of the serotonergic system in suicidal behavior. J Psychi-
atr Res 2003;37:375–386.
49. Baldessarini RJ, Hennen J. Genetics of suicide: an over-
view. Harv Rev Psychiatry 2004;12:1–13.
50. Bellivier F, Chaste P, Malafosse A. Association between
the TPH gene A218C polymorphism and suicidal
behavior: a meta-analysis. Am J Med Genet B Neuro-
psychiatr Genet 2004;124:87–91.
51. Bondy B, Buettner A, Zill P. Genetics of suicide. Mol
Psychiatry 2006;11:336–351.
52. Lalovic A, Turecki G. Meta-analysis of the association
between tryptophan hydroxylase and suicidal behavior.
Am J Med Genet 2002;114:533–540.
53. Li D, He L. Meta-analysis supports association between
serotonin transporter (5-HTT) and suicidal behavior. Mol
Psychiatry 2007;12:47–54.
54. Lin PY, Tsai G. Association between serotonin transporter
gene promoter polymorphism and suicide: results of a
meta-analysis. Biol Psychiatry 2004;55:1023–1030.
55. Rujescu D, Thalmaier A, Mıller H-J, Bronisch T, Giegling
I
. Molecular genetic findings in suicidal behavior: what is
beyond the serotonergic system? Arch Suicide Res
2007;11:17–40.
56. Voracek M, Loibl LM. Genetics of suicide: a systematic
review
of
twin
studies.
Wien
Klin
Wochenschr
2007;119:463–475.
57. Mann JJ, Brent DA, Arango V. The neurobiology and
genetics of suicide and attempted suicide: a focus on the
serotonergic
system.
Neuropsychopharmacology
2001;24:467–477.
58. Mann JJ. Role of the serotonergic system in the patho-
genesis of major depression and suicidal behavior. Neu-
ropsychopharmacology 1999;21:99–105.
59. Souery D, Oswald P, Linkowski P, Mendlewicz J. Molecular
genetics in the analysis of suicide. Ann Med 2003;35:191–
196.
60. Van Heeringen K. The neurobiology of suicide and suici-
dality. Can J Psychiatry 2003;48:292–300.
61. Kaplan SJ, Pelcovitz D, Labruna V. Child and adolescent
abuse and neglect research: a review of the past 10 years.
Part I: physical and emotional abuse and neglect. J Am
Acad Child Adolesc Psychiatry 1999;38:1214–1222.
62. Malinosky-Rummell R, Hansen DJ. Long-term conse-
quences of childhood physical abuse. Psychol Bull
1993;114:68–79.
63. Briere J. The long-term clinical correlates of childhood
sexual victimization. Ann N Y Acad Sci 1988;528:327–334.
64. Wagner B, Silverman M, Martin C. Family factors in
youth suicidal behaviors. Am Behav Sci 2003;46:1171–
1191.
Maniglio
40

65. Joiner Te JR, Brown JS, Wingate LR. The psychology and
neurobiology of suicidal behavior. Annu Rev Psychol
2005;56:287–314.
66. Conner KR, Duberstein PR, Conwell Y, Caine ED. Reac-
tive aggression and suicide: theory and evidence. Aggress
Violent Behav 2003;8:413–432.
67. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a
clinical model of suicidal behavior in psychiatric patients.
Am J Psychiatry 1999;156:181–189.
68. Brezo J, Paris J, Turecki G. Personality traits as correlates
of suicidal ideation, suicide attempts, and suicide
completions: a systematic review. Acta Psychiatr Scand
2006;113:180–206.
69. Glanz LM, Haas GL, Sweeney JA. Assessment of hopeless-
ness in suicidal patients. Clin Psychol Rev 1995;15:49–64.
70. Yen S, Shea MT, Sanislow CA et al. Personality traits as
prospective predictors of suicide attempts. Acta Psychiatr
Scand 2009;120:222–229.
71. Pinikahana J, Happell B, Keks NA. Suicide and schizo-
phrenia: a review of literature for the decade (1990–1999)
and implications for mental health nursing. Issues Ment
Health Nurs 2003;24:27–43.
72. Reid S. Suicide in schizophrenia. A review of the litera-
ture. J Ment Health 1998;7:345–353.
73. Arsenault-Lapierre G, Kim C, Turecki G. Psychiatric
diagnoses in 3275 suicides: a meta-analysis. BMC Psy-
chiatry 2004;4:37–47.
74. Isometsa ET. Psychological autopsy studies: a review. Eur
Psychiatry 2001;16:379–385.
75. Wolfsdorf BA, Freeman J, Deramo K, Oveholser J, Spirito
A
. Mood states: depression, anger, and anxiety. In: Spirito
A
, Overholser JC, eds. Evaluating and treating adolescent
suicide attempters: from research to practice. New York:
Academic, 2003:55–81.
76. Rihmer Z. Suicide risk in mood disorders. Curr Opin
Psychiatry 2007;20:17–22.
77. Pompili M, Girardi P, Ruberto A, Tatarelli R. Suicide in
borderline personality disorder: a meta-analysis. Nord J
Psychiatry 2005;59:319–324.
78. Blasco-Fontecilla H, Baca-Garcia E, Dervic K et al.
Severity of personality disorders and suicide attempt.
Acta Psychiatr Scand 2009;119:149–155.
79. Bagge CL, Sher KJ. Adolescent alcohol involvement and
suicide attempts: toward the development of a conceptual
frame work. Clin Psychol Rev 2008;28:1283–1296.
80. Esposito-Smythers C, Spirito A. Adolescent suicidal behav-
ior and substance use: a review with implications for
treatment research. Alcohol Clin Exp Res 2004;28:77–88.
81. Hufford MR. Alcohol and suicidal behavior. Clin Psychol
Rev 2001;21:797–811.
82. Mehlenbeck R, Spirito A, Barnett N, Overholser J.
Behavioral factors: substance use. In: Spirito A, Over-
holser JC
, eds. Evaluating and treating adolescent suicide
attempters: from research to practice. San Diego, CA:
Academic Press, 2003:113–146.
83. Franko DL, Keel PK. Suicidality in eating disorders:
occurrence, correlates, and clinical implications. Clin
Psychol Rev 2006;26:769–782.
84. Pompili M, Mancinelli I, Girardi P, Ruberto A, Tatarelli R.
Suicide in anorexia nervosa: a meta-analysis. Int J Eat
Disord 2004;36:99–103.
85. Hawton K, Sutton L, Haw C, Sinclair J, Harriss L. Suicide
and attempted suicide in bipolar disorder: a systematic
review of risk factors. J Clin Psychiatry 2005;66:693–704.
86. Kilbane EJ, Gokbayrak NS, Galynker I, Cohen L, Tross S.
A review of panic and suicide in bipolar disorder: does
comorbidity increase risk? J Affect Disord 2009;115:1–10.
87. Post RM, Leverich GS, Xing G, Weiss SB. Developmental
vulnerabilities to the onset and course of bipolar disorder.
Dev Psychopathol 2001;13:581–598.
88. Sa´nchez-Gistau V, Colom F, Mane´ A, Romero S, Sugranyes
G
, Vieta E. Atypical depression is associated with suicide
attempt in bipolar disorder. Acta Psychiatr Scand
2009;120:30–36.
89. James A, Lai FH, Dahl C. Attention deficit hyperactivity
disorder and suicide: a review of possible associations.
Acta Psychiatr Scand 2004;110:408–415.
90. Panagioti M, Gooding P, Tarrier N. Post-traumatic stress
disorder and suicidal behavior: a narrative review. Clin
Psychol Rev 2009;29:471–482.
91. Briere J, Elliot DM. Sexual abuse, family environment,
and psychological symptoms: on the validity of statistical
control. J Consult Clin Psychol 1993;61:284–288.
92. Sheldrick C. Adult sequelae of child sexual abuse. Br J
Psychiatry 1991;158:55–62.
93. Brent DA, Mann JJ. Family genetics studies, suicide, and
suicidal behavior. Am J Med Genet C Semin Med Genet
2005;133:13–24.
94. Mann JJ. Neurobiology of suicidal behaviour. Nat Rev
Neurosci 2003;4:819–828.
95. Baud P. Personality traits as intermediary phenotypes in
suicidal behavior. Am J Med Genet C Semin Med Genet
2005;133:34–42.
96. Klonsky ED. The functions of deliberate self-injury: a
review of the evidence. Clin Psychol Rev 2007;27:226–
239.
97. Connors R. Self-injury in trauma survivors: functions and
meanings. Am J Orthopsychiatry 1996;66:197–206.
98. Stanley B, Winchel R, Molcho A, Simeon D, Stanley M.
Suicide and the self-harm continuum: phenomenological
and biochemical evidence. Int Rev Psychiatry 1992;4:149–
155.
99. Suyemoto KL. The functions of self-mutilation. Clin Psy-
chol Rev 1998;18:531–554.
100. Maniglio R. Severe mental illness and criminal victimiza-
tion:
a
systematic
review.
Acta
Psychiatr
Scand
2009;119:180–191.
101. Maniglio R. The role of deviant sexual fantasy in the
etiopathogenesis of sexual homicide: a systematic review.
Aggress Violent Behav 2010;15:294–302.
Child sexual abuse and self-injury
41

Copyright of Acta Psychiatrica Scandinavica is the property of Wiley-Blackwell and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.
Wyszukiwarka
Podobne podstrony:
Severity of child sexual abuse and revictimization The mediating role of coping and trauma symptoms
MMPI 2 F Scale Elevations in Adult Victims of Child Sexual Abuse
The Role of Seeing Blood in Non Suicidal Self Injury
Co existence of GM and non GM arable crops the non GM and organic context in the EU1
The Role of Trust and Contractual Safeguards on
How Did You Feel Increasing Child Sexual Abuse Witnesses Production of Evaluative Information
Resistance to organizational change the role of cognitive and affective processes
The Roles of Gender and Coping Styles in the Relationship Between Child Abuse and the SCL 90 R Subsc
Newell, Shanks On the Role of Recognition in Decision Making
Morimoto, Iida, Sakagami The role of refections from behind the listener in spatial reflection
86 1225 1236 Machinability of Martensitic Steels in Milling and the Role of Hardness
ROLE OF THE COOPERATIVE BANK IN EU FUNDS
Illiad, The Role of Greek Gods in the Novel
Hippolytus Role of Greek Gods in the Euripedes' Play
The Role of the Teacher in Methods (1)
THE ROLE OF CATHARSISI IN RENAISSANCE PLAYS - Wstęp do literaturoznastwa, FILOLOGIA ANGIELSKA
The Role of Women in the Church
The Role of the Teacher in Teaching Methods
więcej podobnych podstron