What do British women know about cervical cancer symptoms
and risk factors?
q
Emma L. Low
, Alice E. Simon
, Jane Lyons
, Debbie Romney-Alexander
Jo Waller
a
Cancer Research UK Health Behaviour Research Centre, Department of Epidemiology and Public Health, University College London,
1–19 Torrington Place, London WC1E 6BT, UK
b
Formerly of The Eve Appeal, Butler House, 177–178 Tottenham Court Road, London W1T 7NY, UK
c
Department of Health England (Cancer Team), Department of Health, Richmond House 79 Whitehall, London SW1A 2NS, UK
Available online 7 June 2012
KEYWORDS
Cervical cancer
Risk factor awareness
Symptom awareness
Cancer knowledge
Abstract
Objective: To identify levels of cervical cancer risk factor and symptom awareness,
as well as predictors of higher awareness in a United Kingdom (UK) female population.
Design: Population based survey.
Setting: Participants’ homes in the UK.
Sample: UK representative sample of females aged 16 years and over (n = 1392).
Materials and methods: Respondents completed the Cervical Cancer Awareness Measure
which included questions on awareness of cervical cancer symptoms and risk factors (both
recalled and recognised). Linear regression analyses were used to identify predictors of higher
symptom and risk factor recognition scores.
Main outcome measures: Awareness of cervical cancer symptoms and risk factors.
Results: Sixty-five percent of respondents were unable to recall any risk factors and 75% were
unable to recall any symptoms. Awareness was higher when women were prompted (95%
recognised at least one risk factor and 93% at least one symptom). Independent predictors
of risk factor recognition were older age and higher education. Symptom recognition was
associated with older age, White ethnicity, higher education and having a close experience
of cervical cancer.
Conclusions: To reduce inequalities in awareness, interventions should target younger women
with lower education and those from ethnic minority groups.
Ó 2012 Elsevier Ltd. All rights reserved.
0959-8049/$ - see front matter
Ó 2012 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ejca.2012.05.004
q
The views expressed in this paper are those of the individual authors and not of the Department of Health.
⇑
Corresponding author: Tel.: +44 (0) 20 7679 1736; fax: +44 (0) 20 7679 8354.
E-mail address:
(E.L. Low).
European Journal of Cancer (2012) 48, 3001– 3008
A v a i l a b l e a t
w w w . s c i e n c e d i r e c t . c o m
j o u r n a l h o m e p a g e : w w w . e j c a n c e r . i n f o

1. Introduction
Cervical cancer mortality rates have dropped by
almost 70% since 1979.
This fall can be attributed to
the introduction of the national cervical cancer screen-
ing programme in 1988, a call-recall programme
designed to detect potentially cancerous abnormalities
in the cervix.
In 2008, the National Health Service
(NHS) also implemented a national Human Papilloma-
virus (HPV) vaccination programme designed to protect
women against infection with HPV types 16 and 18 (the
cause of up to 71% of cervical cancer cases).
HPV vaccines have a very high preventative efficacy
rate,
meaning that almost all vaccinated girls will be
protected against three-quarters of incidences of cervi-
cal cancer. The vaccine is currently offered to girls
aged 12–13 (a three-year ‘catch-up’ programme was
also run in addition to the main programme for girls
aged 14–18 in 2008). However, as cervical cancer is
most common in women aged 30–39
the effects of
the vaccine on incidence will not be evident until the
vaccinated girls near this age (although we should
see a marked drop in abnormal cytology earlier as
women are offered screening from age 25 in the
United Kingdom (UK)).
Around a quarter of the routine vaccination cohort
(girls aged 12–13 years) did not complete the three-dose
HPV vaccination course (required for full protection) in
the academic year 2009–2010, according to latest fig-
ures.
Further, the vaccine only protects against the
HPV types responsible for three quarters of cervical can-
cers,
therefore, even if vaccinated, women are not fully
protected from cervical cancer. For women who do con-
tract a high-risk HPV not covered by the vaccine, the
screening programme should detect any resulting cell
abnormalities, reducing the chances of these developing
into cervical cancer. However, almost 30% of cervical
cancers occur in women who appeared to have been
fully adherent to the screening programme.
Although there has been a decline, there were still-
around 950 deaths attributable to cervical cancer per
year in the UK between 2006 and 2008.
As England
and Wales have a significantly lower survival rate than
the European mean,
there may be room for improve-
ment in cervical cancer survival rates in the UK. To
achieve this, it is important to identify modifiable factors
that could increase the likelihood of survival.
Cervical cancer diagnoses made at an earlier stage
(FIGO (International Federation of Gynecology and
Obstetrics) stages 1A1 to 1B2) are associated with higher
survival rates (80–99%) than diagnoses made at a later
stage (stages III–IV have associated five-year survival
rates of 20–50%).
At present, in England, almost
10% of cervical cancers are diagnosed at stage III or
worse.
If this figure can be decreased, cervical cancer
mortality can be further reduced.
Early-stage cervical cancer diagnoses may result from
prompt medical help-seeking in the presence of symp-
toms,
itself associated with factors such as symptom
and risk factor awareness.
By determining levels
of awareness of cervical cancer risk factors and symp-
toms in the UK population, we can identify areas of
poor knowledge that could be targeted in health educa-
tion programmes.
There are a number of risk factors for the develop-
ment of cervical cancer, varying in importance. While
the key risk factor is infection with high-risk HPV (as
this is a necessary cause of almost all cervical cancers),
it could be argued that irregular attendance at cervical
screening is a more important risk factor for women
to understand, as screening behaviour is likely to be eas-
ier to modify than behaviours that affect the risk of
acquiring an HPV infection.
In 2007, Marlow et al.
tested unprompted recall of
several risk factors for cervical cancer (including not
going for regular screening) and prompted recognition
of HPV. Recall was low for all of the risk factors,
including HPV (3%) and not going for regular screening
(5%) and even when prompted, only 24% of participants
endorsed HPV.
In another earlier study, Wardle et al.
investigated
prompted awareness of risk factors for cancer, including
three cervical cancer risk factors (having many sexual
partners, having a virus or infection and smoking). Rec-
ognition, though higher than the recall in Marlow
et al.’s study, was fairly low for two of the three risk fac-
tors. Higher awareness of some cervical cancer risk fac-
tors has been associated with more education,
younger age and White ethnicity.
Further, a personal
or family history of cancer has been associated with
higher awareness of cancer in general.
As with risk factors, there are some symptoms of cer-
vical cancer that are more important than others. The
most important symptoms of cervical cancer are unusual
vaginal bleeding and persistent vaginal discharge that is
blood-stained or smells unpleasant. These are the most
common
and, in the case of unusual vaginal bleeding,
may be more likely to be present in earlier stage dis-
ease.
In the UK there has not yet been a systematic
attempt to assess population levels of cervical cancer
symptom awareness, either for these common symptoms
or for the less important symptoms, although there is
evidence that cancer symptom awareness in general is
low in UK women.
Predictors of higher symptom awareness include
older age, White ethnicity and higher socioeconomic sta-
tus (SES).
There is also evidence that knowing close
family or friends who have experienced cancer can
increase awareness of some symptoms of cancer.
The data in the current study were collected just prior
to the launch of the Department of Health’s key messages
on cervical cancer in 2010.
By measuring awareness at
3002
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
this point in time, we can allow for a comparison of
awareness post-introduction of these messages, therefore
ascertaining the impact of the key messages on women’s
awareness of cervical cancer symptoms.
In the present study we aimed to determine cervical
cancer risk factor and symptom awareness in a UK
female population. We hypothesised that higher educa-
tion level (a commonly used marker of SES (e.g. Ref.
), having a personal or close experience of cervical
cancer and White ethnicity would predict higher risk
factor and symptom awareness. We also expected that
older age would be associated with symptom awareness,
but that younger age would be associated with risk fac-
tor awareness.
2. Materials and methods
2.1. Recruitment
UK females aged 16 years and over were recruited
through a social research agency (TNS-BMRB) using
random location sampling. Women who did not speak
English were excluded from participation in the survey.
As part of TNS-BMRB’s omnibus survey, 1392 women
self-completed the Cervical Cancer Awareness Measure
(Cervical CAM)
(a site-specific version of the generic
CAM),
at home using Computer Assisted Personal
Interviewing (CAPI) in the presence of fully trained
interviewers. Data were collected between November
and December 2009.
2.2. Sample characteristics
The number of non-White participants was very small
for each ethnic background, so we grouped respondents
from non-White ethnic backgrounds together, dichoto-
mising the women into ‘White’ or ‘non-White’. White
non-British women were included in the ‘White’ cate-
gory. An adequate level of spoken English to understand
the survey was a pre-requisite for participation. Educa-
tion was grouped into ‘Low-level/none’ (women edu-
cated to ONC, BTEC, O Level/GCSE A–G (ie
academic examinations normally taken at age 16 years
in the UK) and those with no formal education),
‘Mid-level’ (women educated to A Levels/Highers, higher
education below degree (ie academic examinations nor-
mally taken at age 18 years in the UK) and those who
answered ‘other’ or were still studying) and ‘High-level’
(degree level or higher). Women who answered ‘other’
were placed into the ‘Mid-level’ education group as pre-
liminary analysis (not reported here) revealed that they
had similar levels of recall and recognition to the other
education level categories in that group. Age was
measured as a continuous variable.
We asked respondents whether they had had cervical
cancer and/or whether they had known a close family
member or friend with cervical cancer. Respondents
scored ‘1’ if they had and ‘0’ if they had not.
2.3. Awareness of risk factors
We measured risk factor awareness with both open
and closed questions. The open question (presented
before the closed question to reduce bias) measured
recall and read: ‘What things do you think affect a
woman’s
chance
of
developing
cervical
cancer?’.
Respondents were given a blank space to freely respond.
The closed question (measuring recognition) read:
‘The following may or may not increase the chance of
getting cervical cancer. How much do you agree or dis-
agree that the following can increase the chance of get-
ting cervical cancer?’. Participants were presented with
10 cervical cancer risk factors and response options:
‘Strongly agree’, ‘Agree’ (scored ‘1’), ‘Neither agree
nor disagree’, ‘Disagree’ or ‘Strongly disagree’ (scored
‘0’). A refusal to answer was coded as ‘missing’.
For the open question, participants scored ‘1’ for
each risk factor mentioned that corresponded with the
list in the closed question (target risk factors) for ease
of comparison (see
for the full list). Scores from
the open and closed questions were each summed to cre-
ate an overall score for recall and for recognition (range
for both questions = 0–10).
We also measured how many women responded with
any risk factors that wouldn’t be deemed ‘incorrect’, but
did not match the target list in the closed question. Con-
sequently, we added two additional risk factors to the
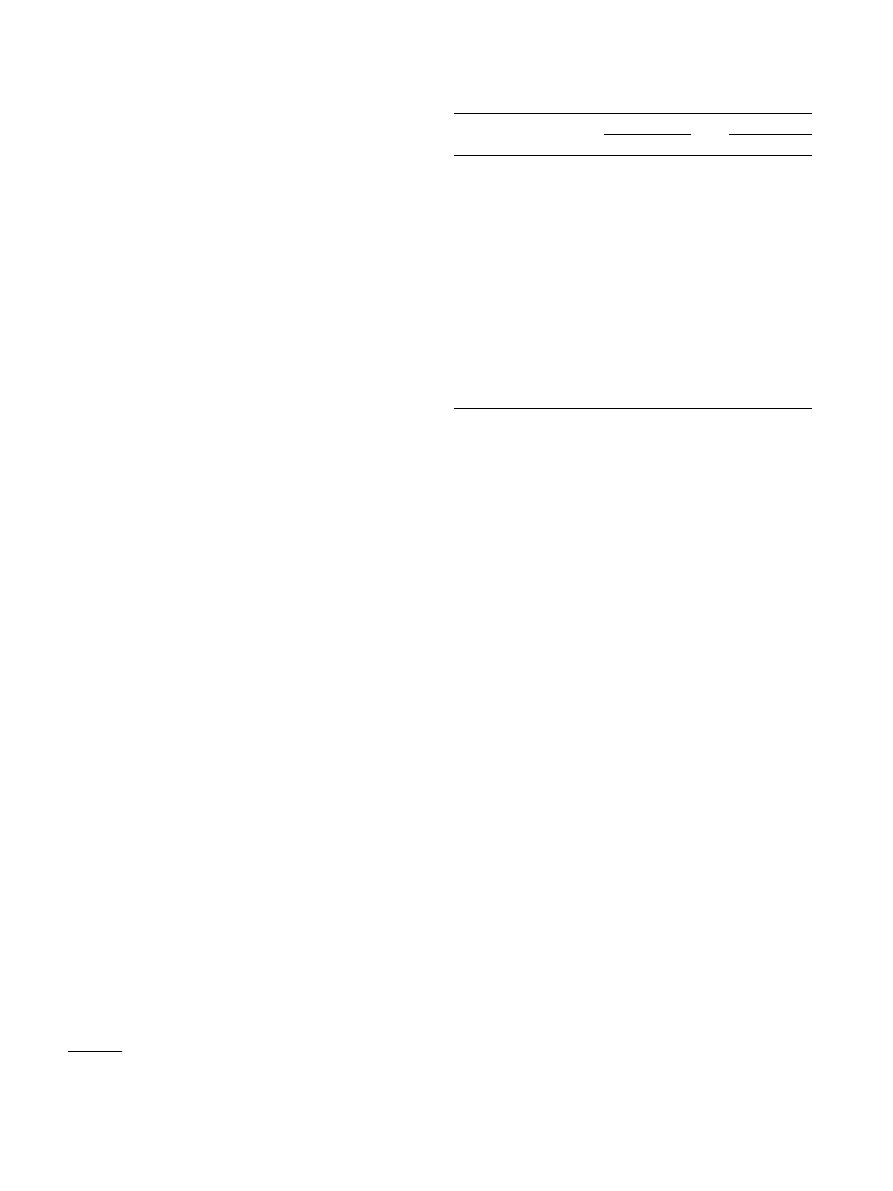
Table 1
Sample characteristics (weighted/unweighted n = 1392).
Unweighted
Weighted
N
%
N
%
Age
16–24
158
11.4
208
14.9
25–39
425
30.5
343
24.7
40–59
416
29.9
431
30.9
60+
393
28.2
410
29.5
Ethnicity
White
1240
89.1
1261
90.6
Non-White
149
10.7
128
9.2
Education
High-level
256
18.4
285
20.5
Mid-level
230
16.5
233
16.8
Low-level/none
749
53.8
705
50.7
Close experiences of cancer
No-one
1171
84.1
1179
84.7
At least one person
221
15.9
213
15.3
a
Where % < 100%, this is due to missing data.
d
The full Cervical Cancer Awareness Measure can be downloaded
from the NAEDI (National Awareness and Early Detection initiative)
website at
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
3003
‘recalled’ list. Respondents received a score of ‘1’ if they
mentioned ‘Infection/STI/STD or virus’ and if they
mentioned ‘unprotected sex’. Otherwise, they received
a score of ‘0’.
2.4. Awareness of symptoms
We measured symptom recall using the question:
‘There are several warning signs and symptoms of cervi-
cal cancer. Please type in as many as you can think of’.
Participants were presented with a blank space for
responses.
Again, we measured recognition with a closed ques-
tion: ‘The following may or may not be warning signs
for cervical cancer. We are interested in your opinion’.
Participants were presented with 11 symptoms of cervi-
cal cancer and offered response options ‘Yes’, ‘No’ or
‘Don’t know’, as well as the option to refuse to answer
the question. If participants chose this option, their data
were coded as ‘missing’.
For each symptom, a ‘Yes’ response scored ‘1’.
Responses ‘No’ and ‘Don’t know’ scored ‘0’. To allow
comparisons between recall and recognition scores,
recalled symptoms that corresponded with the list of
11 symptoms in the closed question (target symptoms)
(see
for the full list) were scored as ‘recalled’
(‘1’) if they were mentioned. Scores from each question
were summed to give a total ‘recall’ score and a total
‘recognition’ score (range for both questions = 0–11).
Finally, we measured how many women responded
with any non-specific reference to vaginal bleeding
(including ‘irregular bleeding’/‘spotting’/‘non-specific
bleeding’) in the open question as, although these
answers do not specifically relate to the closed question
responses, they are not ‘incorrect’. If a respondent men-
tioned at least one of these symptoms, they received a
score of ‘1’. Otherwise, they received a score of ‘0’.
2.5. Analyses
Data were analysed using SPSS version 19. We ran
multiple linear regressions to determine independent
predictors of awareness (recognition) of symptoms and
risk factors. Recall and recognition of cancer symptoms
have been shown to have similar correlates; however,
recognition levels are usually considerably higher than
recall.
As some symptoms had a recall rate of zero,
it was easier to determine group differences by using rec-
ognition scores in the regression analyses. Further,
CAM symptom recognition scores have been shown to
be an independent predictor of time to help-seeking.
For both regression models we entered age, ethnicity,
education level and experience of cervical cancer as pre-
dictor variables. Data were weighted using a rim weight-
ing technique, in which target profiles were set for five
separate demographic variables (occupational status,
parity, age group, social grade and geographical region)
to achieve a demographic profile within the sample
which was representative of women aged 16 and over
in England.
3. Results
3.1. Sample characteristics
The sample consisted of 1392 women.
details
the sample characteristics, showing both weighted and
unweighted data. Weighting had the biggest effect on
age groups, with the youngest group over-represented
and those aged 25–39 under-represented. The remaining
variables
had marginal differences.
Characteristics
reported here use the weighted data. Participants were
aged 16–94 (M = 47 years). Most were from White eth-
nic backgrounds (91%) and either had no formal educa-
tion or were educated to a low level (51%). The majority
of participants had not had cervical cancer themselves,
nor had they known anyone close to them who had
(85%).
3.2. Awareness of risk factors
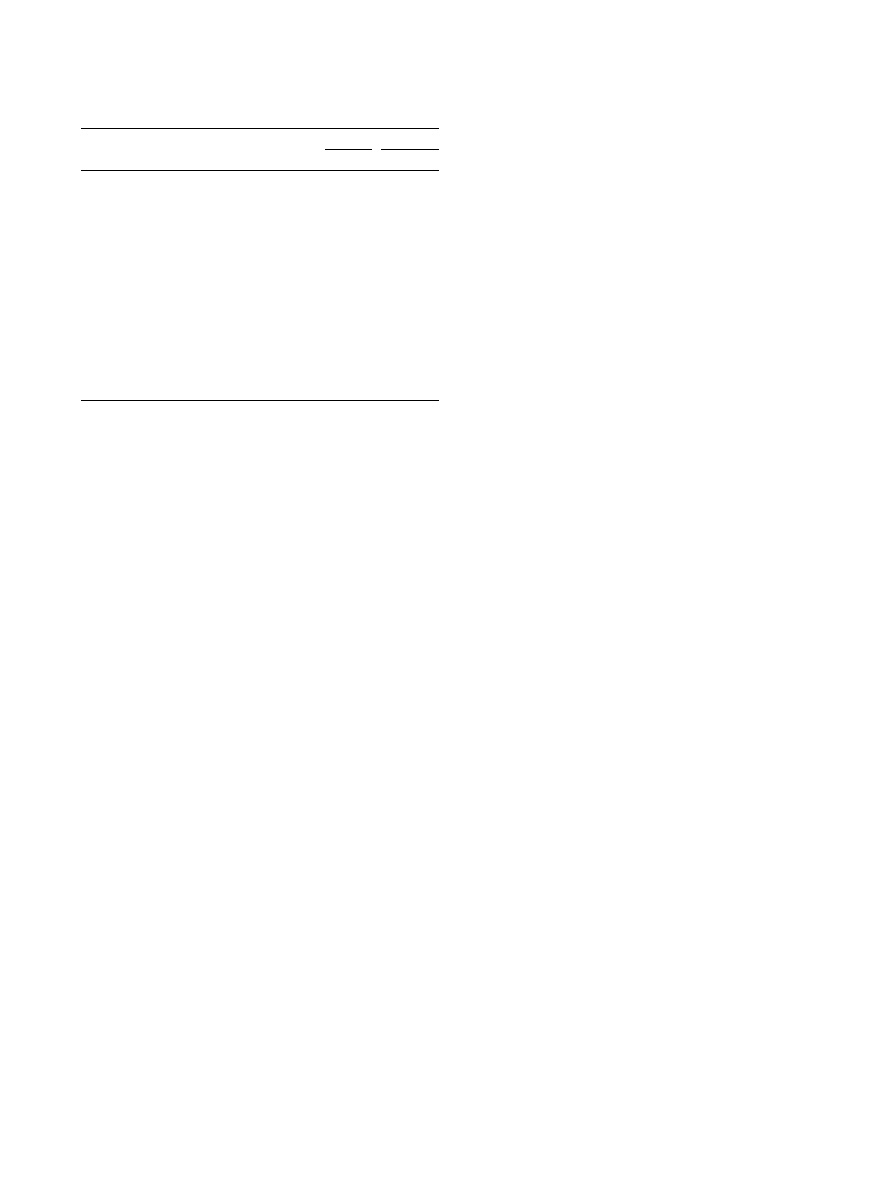
Two-thirds of respondents (65%, n = 905) were
unable to recall any of the target risk factors
(M = 0.44, SD = 0.67). The remainder (35%, n = 487)
correctly recalled at least one. ‘Having many sexual
partners’ was the most recalled target risk factor
(20%). The least recalled were ‘having many children’
(0.2%) and ‘having a weakened immune system (e.g.
because of HIV/AIDS, immunosuppressant drugs or
having a transplant)’ (0.1%). Mean recall score was
slightly higher (M = 0.52, SD = 0.78) when open
responses ‘Infection/STI/STD or virus’ (recalled by
1%) and ‘unprotected sex’ (recalled by 7%) were
included.
Table 2
Number of recalled and recognised cervical cancer risk factors
(weighted n = 1392).
Risk factor
Recalled
Recognised
(n)
%
(n)
%
Having many sexual partners
272 19.5
884 63.5
Smoking any cigarettes
121
8.7
706 50.7
Starting to have sex at a young age
111
8.0
758 54.4
Unprotected sex
101
7.3
–
–
Not going for regular smear (Pap) tests
78
5.6 1046 75.2
Infection, STI/STD or virus
20
1.4
–
–
Infection with Chlamydia
19
1.4
748 53.7
Infection with Human Papillomavirus (HPV)
15
1.1
643 46.2
Long term use of the contraceptive pill
4
0.3
460 33.0
Having a sexual partner with many previous
partners
4
0.3
740 53.1
Having many children
3
0.2
167 12.0
Having a weakened immune system (e.g.
because of HIV/AIDS, immunosuppressant
drugs or having a transplant)
2
0.1
692 49.7
3004
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
Awareness was substantially higher when measured
by recognition (with 95% able to identify at least one
risk factor), however on average women still only cor-
rectly identified half of the risk factors presented
(M = 4.96/10, SD = 2.50). The most recognised risk fac-
tors were ‘Not going for regular smear (Pap) tests’ (75%)
and ‘Having many sexual partners’ (64%). The least
recognised was ‘having many children’ (12%) (
When risk factor recognition score was regressed
onto the demographic and cancer experience variables
the model accounted for a small but significant propor-
tion of the variance (Adj. R
2
= 0.02, F(4,1366) = 9.48,
p < 0.001). Older age and a higher level of education
significantly predicted higher awareness of cervical can-
cer risk factors in the model. The effect size was similar
for age (gp
2
= 0.02, p < 0.001) and education level
(gp
2
= 0.02, p < 0.001) (
3.3. Awareness of symptoms
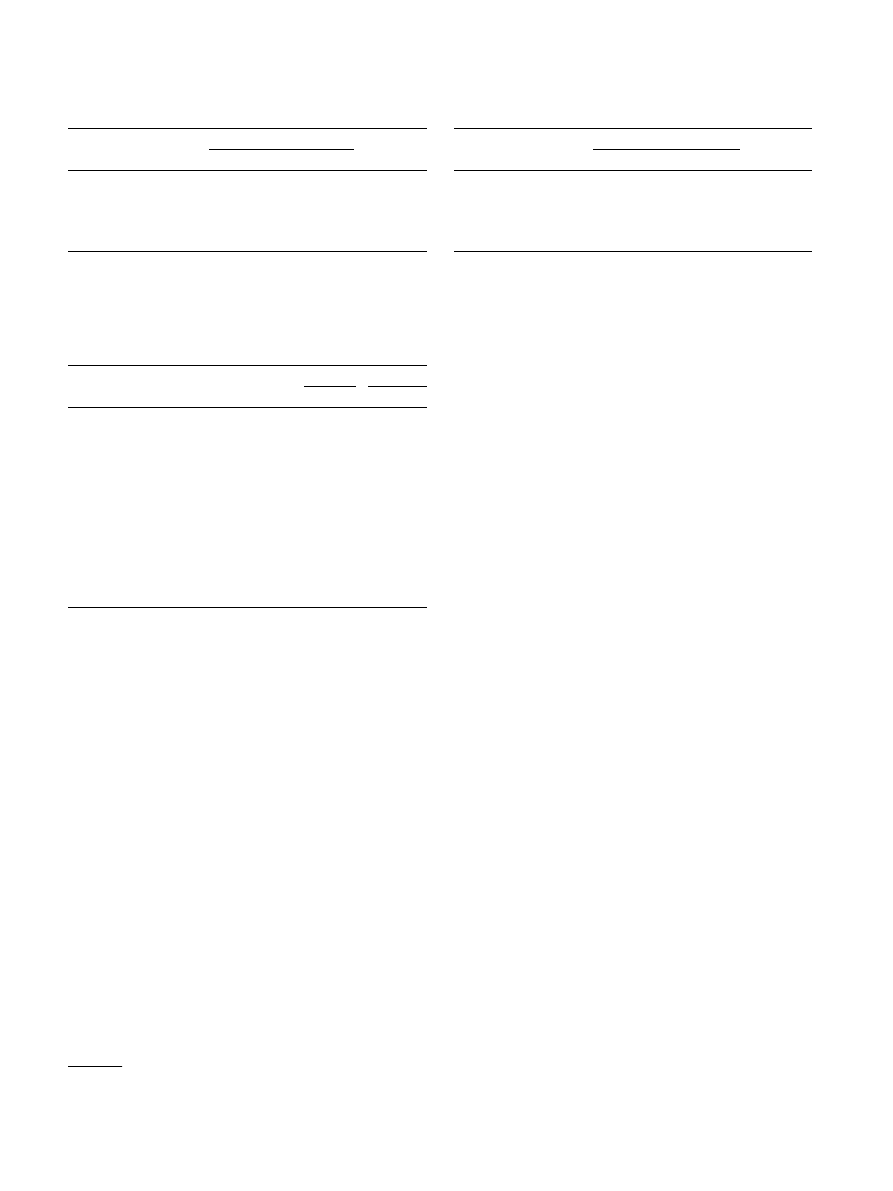
Two-thirds of the women were unable to recall any of
the target symptoms (75%, n = 1049). This figure was
lower (55%, n = 764) when responses ‘irregular bleed-
ing’/‘spotting’/‘non-specific
bleeding’
were
included
(M = 0.59, SD = 0.77). Recognition was better than
recall, with 93% correctly recognising at least one symp-
tom of cervical cancer (M = 6.08/11, SD = 2.85).
Although not on the target list, unusual vaginal
bleeding (including responses: ‘irregular bleeding’/‘spot-
ting’/‘non-specific bleeding’) was the most recalled
symptom of cervical cancer (29%), followed by ‘persis-
tent, abnormal or unusual vaginal discharge’ (15%). Pat-
terns were different when women were asked to
recognise symptoms, with recognition highest for ‘vagi-
nal bleeding between periods’ (73%), and ‘persistent pel-
vic pain’ (70%). Few women knew that ‘persistent
diarrhoea’ was a symptom of cervical cancer as it was
both the least recalled (0%) and recognised (12%) symp-
tom (
The multiple regression model explained 4% of the
variance in symptom recognition (Adj R
2
= 0.04,
F(4,1367) = 15.28, p < 0.001). Older age, White ethnic
background, higher level of education and having a
close experience of cervical cancer all predicted higher
cervical cancer symptom recognition. The effect size
was strongest for ethnicity (gp
2
= .03, p < 0.001) and
education level (gp
2
= .01, p < 0.001) and weaker for
age (gp
2
= .01, p < 0.01) and close experience of cervical
cancer (gp
2
= .01, p < 0.01) (
4. Discussion
Most respondents were unable to recall any symp-
toms or risk factors for cervical cancer. Awareness was
much higher for both when prompted; although even
then women were only able to recognise around half
of the symptoms and risk factors presented.
Although the most recognised risk factor was ‘not
going for regular smear (Pap) tests’ (>75%), a quarter
of women were not able to identify this risk factor even
when prompted. It has been suggested that lack of
awareness of the function of the cervical cancer screening
Table 4
Awareness of cervical cancer symptoms (weighted n = 1392).
Symptom
Recalled
Recognised
(n)
%
(n)
%
Unusual vaginal bleeding
397
28.5
-
-
Persistent/abnormal/unusual vaginal
discharge
202
14.5
861
61.9
Vaginal bleeding between periods
61
4.4
1020
73.3
Heavier/longer periods than normal
46
3.3
723
52.0
Vaginal bleeding during/after sex
32
2.3
886
63.7
Pain/discomfort during sex
28
2.0
864
62.0
Persistent pelvic pain
20
1.4
971
69.8
Unexplained weight loss
14
1.0
778
55.9
Blood in stool/urine
12
0.9
598
43.0
Persistent lower back pain
11
0.8
602
43.3
Vaginal bleeding after the menopause
4
0.3
923
66.3
Persistent diarrhoea
0
0.0
164
11.8
a
This includes any reference in the open responses to non-specific
vaginal bleeding, including ’irregular bleeding’/‘spotting’/‘non-specific
bleeding’ that did not match with the target symptoms in the closed
question.
Table 3
Regression for predictors of cervical cancer risk factor knowledge
(recognised) (weighted n = 1372).
B
95% confidence interval (CI) SE
b
Lower
Upper
Constant
3.69
3.07
4.31
0.32
Age
0.02
0.01
0.02
0.00
Ethnicity
0.24
0.70
0.22
0.24
0.03
Education
0.40
0.23
0.57
0.09
Cancer experience
0.27
0.09
0.63
0.18
0.04
a
Significant at 0.001.
Table 5
Regression for predictors of cervical cancer symptom recognition
(weighted n = 1373).
B
95% confidence interval (CI)
SE
b
Lower
Upper
Constant
3.55
2.85
4.25
0.36
Age
0.01
0.00
0.02
0.00
Ethnicity
1.46
0.94
1.98
0.26
Education
0.43
0.24
0.62
0.10
Cancer experience
0.56
0.16
0.97
0.21
a
Significant at 0.01.
b
Significant at 0.001.
e
Analyses (not reported here) showed that the relationship was the
same when the ‘other’ education group was not included.
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
3005

programme can negatively affect attendance.
Currently
around 20% of eligible women are not participating in
screening
; and coverage for women in the higher risk
age group (25–49 years) is falling.
Increasing awareness
that the cervical screening programme can reduce the
risk of cervical cancer may help to increase attendance,
resulting in lower incidence and consequently mortality.
Recognition of ‘smoking’ (51%) and ‘infection with
Chlamydia’ (54%) as risk factors for cervical cancer
appears to have improved in our study compared to ear-
lier research,
with over 50% of respondents able to rec-
ognise each. It was disappointing, however, that
awareness of HPV in particular was very low and that,
despite the introduction of the HPV vaccine in 2008
and the associated publicity, awareness of this risk fac-
tor was lower in the current survey than it was reported
to be in a survey carried out in 2006.
Unprompted awareness that having many sexual
partners is a risk factor for cervical cancer was much
higher (20%) than it was for HPV, suggesting that
although many women know there is a link between cer-
vical cancer and sex, the mechanism for this (i.e. HPV
infection) has yet to understood by most. Previous
research on public understanding of the link between
cervical cancer and smoking has highlighted the impor-
tance of having a coherent model linking a risk factor to
an outcome.
Future research might investigate ways of
helping women understand the role of sexual activity in
cervical cancer aetiology.
In contrast to our hypothesis, we found that younger,
not older women had lower awareness of risk factors for
cervical cancer. This is concerning, as incidence is high-
est in women aged 30–34
and there is evidence that
younger women may be more vulnerable to some risk
factors such as infection with Chlamydia.
One expla-
nation of our findings may be our use of a composite
risk factor score, whereas previous research has investi-
gated awareness of individual risk factors for cervical
cancer
or cancer risk factors in general.
A compos-
ite score may lead to higher awareness in older women
as younger women may be more aware of specific risk
factors (such as HPV)
but less aware of risk factors
overall.
The most recalled symptoms in our sample were
‘unusual vaginal bleeding’ (29%) and ‘persistent/abnor-
mal/unusual vaginal discharge’ (15%). This was particu-
larly reassuring given that they are the most common
symptoms of cervical cancer and are highlighted in the
Department of Health’s key messages.
However, less
reassuring was the fact that most women were unable
to recall any symptoms and even for these common
symptoms recall was still quite low.
Recognition was good for the ‘bleeding’ and ‘pain’
symptoms (
), reflecting earlier findings that,
when participants were presented with symptoms of
cancer more generally, two of the three most recalled
symptoms were bleeding and pain symptoms.
This
suggests that women think of cervical cancer symptoms
as relatively alarming or dramatic. As they are not nec-
essarily so, it may be useful to raise awareness of the less
dramatic or vaguer symptoms of cervical cancer (such as
‘unusual vaginal discharge’ as recognition was not as
high for this common symptom (62%) as it was for the
bleeding symptoms).
Studies of help-seeking behaviour support this con-
clusion. They have shown that women are more likely
to seek help promptly for gynaecological cancers if they
perceive their symptom to be alarming (e.g. bleeding) or
serious (e.g. pain) and that they are less likely to seek
help promptly for cancer symptoms in general if they
experience a symptom which is perceived as more com-
mon or vague.
As expected, White ethnicity and higher education
predicted higher recognition of symptoms, reflecting
earlier research for cancer symptoms in general.
We
know that lower SES and non-White women have
poorer outcomes when diagnosed with cancer.
We
also know that GPs are less likely to refer these groups
of women to secondary care.
If women are unaware of
the symptoms for cervical cancer, they may be less likely
to insist on referral for further investigation. Increasing
awareness in these groups could ultimately affect sur-
vival rates by increasing confidence when seeking help
for symptoms, and thus increasing referrals for these
women.
4.1. Strengths and limitations
We used a validated tool to systematically measure
both risk factor and symptom awareness for cervical
cancer, making the task of assessing changes in aware-
ness over time easier. These data were collected just
prior to the launch of the cervical cancer key messages;
using the cervical CAM to assess awareness again in the
future may give an indication of the impact of these key
messages on awareness.
An important limitation was that although we identi-
fied some variables that significantly predicted both risk
factor and symptom awareness, the total amount of var-
iance explained by each model was very small, suggest-
ing that there are other, stronger influences on
awareness that we have not included in our analyses.
Further work should be carried out to identify these
variables.
A final limitation of this study was that, as the sample
was population representative, the proportion of non-
White participants was inevitably small. Given that
women from non-White backgrounds had lower symp-
tom awareness than White women, we feel that ethnic
differences in awareness should be explored in future
studies, which should include a higher proportion of
non-White participants.
3006
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008

5. Conclusions
Awareness of both risk factors and symptoms of cer-
vical cancer was low in UK women. Future research
should investigate awareness of the link between sexual
behaviour, HPV and cervical cancer as our findings sug-
gest that this relationship may not be fully understood.
Some population sub-groups may benefit from more
education on risk factors and symptoms in general –
including younger women, ethnic minorities and those
with less education. It is hoped that by improving
awareness in these groups, prompt help-seeking will be
encouraged, reducing the chances of a poor outcome.
Contribution to authorship
J. Waller, J. Lyons and D. Romney-Alexander con-
ceived of and designed the study, and commissioned
the data collection. E. L. Low, J. Waller and A. Simon
analysed the data. E. L. Low wrote the first draft of the
paper. J. Waller and A. Simon contributed to writing the
paper. All the authors approved the final version of the
manuscript.
Ethical approval
The study was exempt from ethical approval as no
identifying details were collected from the participants.
Conflict of interest statement
None declared.
Acknowledgements/funding
This research was funded by the Department of
Health as part of the Cervical Cancer Awareness and
Symptoms Initiative, a collaborative partnership be-
tween the Department of Health, The Eve Appeal and
the UCL Health Behaviour Research Centre. Jo Waller
and Alice Simon are funded by Cancer Research UK.
Emma Low is funded by an IMPACT studentship
(co-sponsored by UCL, Cancer Research UK and
Target Ovarian Cancer).
References
1. Cancer Research UK. Cervical cancer – UK mortality statistics.
<
http://info.cancerresearchuk.org/cancerstats/types/cervix/mor-
> [accessed Jan 5 2012].
2. Peto J, Gilham C, Fletcher O, Matthews FE. The cervical cancer
epidemic that screening has prevented in the UK. Lancet
2004;364(9430):249–56.
3. Mun˜oz N, Bosch FX, Castellsague´ X, et al. Against which human
papillomavirus types shall we vaccinate and screen? The interna-
tional perspective. Int J Cancer 2004;111(2):278–85.
4. Schiller JT, Castellsague´ X, Villa LL, Hildesheim A. An update of
prophylactic human papillomavirus L1 virus-like particle vaccine
clinical trial results. Vaccine 2008;26:K53–61.
5. NHS Cancer Screening Programmes. NHSCSP Audit of invasive
cervical cancer. National report 2007–2010. <
reening.nhs.uk/cervical/publications/nhscsp-audit-invasive-cer-
vical-cancer-201107.pdf
> [accessed Jan 12 2012].
6. NHS Choices. Cervical screening test. <
tions/cervical-screening-test/pages/introduction.aspx
[accessed
Jan 18 2012].
7. Department of Health. Annual HPV vaccine coverage in England in
2009/2010. Department of Health Publications policy and guidance.
<
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_123795
>;2011 [accessed Jan
5 2012].
8. Office for National Statistics. Cancer incidence and mortality in the
United Kingdom: 2006–2008. <
http://www.ons.gov.uk/ons/rel/
cancer-unit/cancer-incidence-and-mortality/2006-2008/index.html
[accessed Jan 18 2012].
9. Sant M, Allemani C, Santaquilani M, et al. EUROCARE-4.
Survival of cancer patients diagnosed in 1995–1999. Results and
commentary. Euro. J. Cancer 2009;45(6):931–91.
10. Cancer Research UK. Cervical cancer statistics and outlook.
<
http://cancerhelp.cancerresearchuk.org/type/cervical-cancer/treat-
ment/cervical-cancer-statistics-and-outlook#stage
> [accessed Jan 5
2012].
11. Thomson CS, Forman D. Cancer survival in England and the
influence of early diagnosis: what can we learn from recent
EUROCARE results. BJC 2009;101(S2):S102–S109.
12. Kennedy AW, Flagg JS, Webster KD. Gynecologic cancer in the
very elderly. Gynecol Oncol 1989;32(1):49–54.
13. Macleod U, Mitchell ED, Burgess C, Macdonald S, Ramirez AJ.
Risk factors for delayed presentation and referral of symptomatic
cancer: evidence for common cancers. BJC 2009;101(S2):S92–
S101.
14. de Nooijer J, Lechner L, de Vries H. A qualitative study on
detecting cancer symptoms and seeking medical help; an applica-
tion of Andersen’s model of total patient delay. Patient Educ
Couns. 2001;42(2):145–57.
15. de Nooijer J, Lechner L, Candel M, de Vries H. Short- and long-
term effects of tailored information versus general information on
determinants and intentions related to early detection of cancer.
Prev Med 2004;38(6):694–703.
16. Robb K, Stubbings S, Ramirez A, et al. Public awareness of cancer
in
Britain:
a
population-based
survey
of
adults.
BJC
2009;101(S2):S18–S23.
17. Simon A, Waller J, Robb K, Wardle J. Patient delay in
presentation of possible cancer symptoms: the contribution of
knowledge and attitudes in a population sample from the
United Kingdom. Cancer Epidemiol Biomarkers Prev 2010;19(9):
2272–7.
18. Marlow L, Waller J, Wardle J. Public awareness that HPV is a risk
factor for cervical cancer. BJC 2007;97(5):691–4.
19. Wardle J, Waller J, Brunswick N, Jarvis M. Awareness of risk
factors
for
cancer
among
British
adults.
Public
Health
2001;115(3):173–4.
20. Waller J, McCaffery K, Wardle J. Beliefs about the risk factors for
cervical cancer in a British population sample. Prev Med
2004;38(6):745–53.
21. Marlow L, Wardle J, Forster A, Waller J. Ethnic differences in
human papillomavirus awareness and vaccine acceptability. J
Epidemiol Commun Health 2009;63(12):1010–5.
22. Adlard JW, Hume MJ. Cancer knowledge of the general public in
the United Kingdom: survey in a primary care setting and review
of the literature. Clin Oncol 2003;15(4):174–80.
23. NHS Choices. Cervical Cancer – Key messages. <
uk/Conditions/Cancer-of-the-cervix/Pages/Keymessages.aspx
>
[accessed Jan 23 2012].
24. NHS Choices. Cervical Cancer – Symptoms. <
nhs.uk/Conditions/Cancer-of-the-cervix/Pages/Symptoms.aspx
[accessed Apr 24 2012].
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
3007

25. Tabak C, Spijkerman AMW, Verschuren WMM, Smit HA. Does
educational level influence lung function decline (Doetinchem
Cohort Study)? Eur Respir J 2009;34(4):940–7.
26. Simon A, Wardle J, Grimmett C, et al. Ovarian and cervical
cancer awareness: development of two validated measurement
tools. J Fam Plann Reprod Health Care 2011.
http://dx.doi.org/
27. Stubbings S, Robb K, Waller J, et al. Development of a
measurement tool to assess public awareness of cancer. BJC
2009;101(S2):S13–S17.
28. Hansen BT, Hukkelberg SS, Haldorsen T, et al. Factors associated
with non-attendance, opportunistic attendance and reminded
attendance to cervical screening in an organized screening
program: a cross-sectional study of 12,058 Norwegian women.
BMC Public Health 2011;11:264.
29. NHS Information Centre. Cervical Screening Programme, England
2009–10. <
http://www.ic.nhs.uk/statistics-and-data-collections/
screening/cervical-screening/cervical-screening-programme-england-
2009-10
> [accessed Jan 4 2012].
30. NHS Cancer Screening Programmes. NHS Cervical Screening
Programme Annual Review 2011. <
nhs.uk/cervical/publications/cervical-annual-review-2011.pdf
>
[accessed Jan 4 2012].
31. Hall S, Weinman J, Marteau T. The motivating impact of
informing women smokers of a link between smoking and cervical
cancer: the role of coherence. Health Psychol 2004;23(4):419–24.
32. Health Protection Agency. STI Annual Data Tables. <
www.hpa.org.uk/web/HPAweb&Page&HPAwebAutoListName/
Page/1201094610372#4
> [accessed Jan 23 2012].
33. Rachet B, Ellis L, Maringe C, et al. Socioeconomic inequalities in
cancer survival in England after the NHS cancer plan. BJC
2010;103(4):446–53.
34. Jack RH, Davies EA, Moller H. Breast cancer incidence, stage,
treatment and survival in ethnic groups in South East England. Br
J Cancer 2009 Jan 6;100(3):545–50.
35. Morris S, Sutton M, Gravelle H. Inequity and inequality in the use
of health care in England: an empirical investigation. Soc Sci Med
2005;60(6):1251–66.
3008
E.L. Low et al. / European Journal of Cancer 48 (2012) 3001–3008
Document Outline
- What do British women know about cervical cancer symptoms and risk factors?
Wyszukiwarka
Podobne podstrony:
Women s knowledge about cervical cancer
Majchrowska, Anna What do we not know to implement the European Landscape Convention (2010)
What You Need to Know about OCD
What you need to know about Angular 2
What Every Muslim Must Know about Purification
cpumemory Ulrich Drepper What Every Programmer Should Know About Memory
Cervical Cancer Prevention and Early american cancer society
Predictors of perceived breast cancer risk and the relation between preceived risk and breast cancer
Money Management for Women, Discover What You Should Know about Managing Your Money, but Don t!
What do you know when you know a language
1955 What Do the Scriptures Say About “Survival After Death” (Co Pismo Święte mówi o „życiu pozag
2003 05 what do managers know
Bearden Slides Visual Tour of what they don t want you to know about electrical circuits (www chen
What You Must Know About Shelving2
What You Really Need to Know About Moving House with Feng Shui by Jane Purr (2000)
How much do you know about Scotland
New technologies for cervical cancer screening
All you need to know about Telephony and Linux
więcej podobnych podstron