
J Orthop Sci (2006) 11:333–341
DOI 10.1007/s00776-006-1021-1
Original article
Multicenter study for Legg-Calvé-Perthes disease in Japan
Wook-Cheol Kim
1
, Kazuo Hiroshima
2
, and Toshihiko Imaeda
3
1
Department of Orthopaedics, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kawaramachi-Hirokoji,
Kamigyou-ku, Kyoto 602-8566, Japan
2
Department of Orthopaedic Surgery, National Hospital Organization, Osaka National Hospital, Osaka, Japan
3
Department of Public Health, Fujita Health University School of Medicine, Aichi, Japan
Introduction
In Japan, as the number of newborn babies is gradually
decreasing, the incidence of pediatric orthopedic
disease decreases with time. Therefore, the Japanese
Pediatric Orthopaedic Association (JPOA) created a
project team in 2000 to research pediatric orthopedic
disease through a multicenter study. The aim of this
study was to collect epidemiological data on Legg-
Calvé-Perthes disease (LCPD), investigate what treat-
ments for LCPD had been conducted, and the outcomes
of these treatment methods. Using multiple logistic
regression, the risk factors affecting the prognosis of
LCPD were determined.
Material and methods
A survey was sent to approximately 2000 hospitals and
children’s institutions that had been authorized by the
Japanese Orthopaedic Association (JOA). The follow-
ing data were collected for each patient known to have
a diagnosis of LCPD: age, sex, date of diagnosis, family
history, sports history, affected sites, symptoms, loca-
tion of pain, Catterall
1
classification and date of classifi-
cation, Herring
2
classification and date of classification,
date of treatment initiation, treatment methods used
(including whether containment or noncontainment
methods had been used and whether weight-bearing or
non-weight-bearing methods were used if conservative
containment methods had been performed), bracing
period, Stulberg
3
classification and date of evaluation,
and age at last follow-up. The patients in this series were
<
15 years old and were diagnosed as having LCPD dur-
ing January 1, 1993 to December 31, 1995.
In the collected data analysis, one of every two pa-
tients had the same name and same birthday and so was
excluded. For the evaluation of outcome, patients who
had had a hormonal disorder, genetic disorder, and
Abstract
Background. The Japanese Pediatric Orthopaedic Associa-
tion created a project team in 2000 to research pediatric ortho-
pedic disease through a multicenter study. The aim of this
study was to collect epidemiological data on Legg-Calvé-
Perthes disease (LCPD) in Japan.
Methods. The following data were collected by a survey: age,
sex, date of diagnosis, family history, sports history, affected
sites, symptoms, location of pain, Catterall classification,
Herring classification, date of treatment initiation, treatment
methods, bracing period, and Stulberg classification.
Results. A total of 711 patients with 766 affected hips were
seen from January 1, 1993 to December 31, 1995. The average
annual incidence of LCPD was 0.9/100 000. The average age
at diagnosis was 7 years 1 month (2.3–14.3 years). The male/
female ratio of the study population was 6.3 : 1.0. The affected-
side ratio (right hip/left hip/both hips) was 5.1 : 6.8 : 1.0. Both
hips were affected in 7.7% of this series. By the Stulberg
classification there were 211 (69.4%) type I and II patients
(of 304 total patients). Six treatment methods for unilateral
LCPD were compared, and there were no significant differ-
ences in outcome among the six groups. The ordinal logistic
regression analysis showed that the Herring classification, age
at the time of diagnosis, and the affected side (for unilateral
LCPD) were significant predictors. The ordinal logistic regres-
sion analysis also showed that operative treatment had a bet-
ter outcome than conservative treatment, with an odds ratio of
1.872.
Conclusions. Many containment methods for LCPD have
been performed in Japan, and the optimal treatment method
for LCPD was not determined in this study. The overall out-
come, however, was not worse than that in worldwide reports.
Offprint requests to: W.-C. Kim
Received: June 18, 2005 / Accepted: March 9, 2006
334
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
congenital hip disorder were excluded. For the compari-
son of treatment methods, patients who had no Stulberg
evaluation and bilateral LCPD were excluded. Patients
evaluated by the Stulberg classification who were
>
13
years of age or those followed up more than 3.5 years
after diagnosis of LCPD were included in a group to
compare outcomes among treatment methods.
For statistical analysis, the Kruskal-Wallis H test was
used to compare outcomes among treatment methods.
An ordinal logistic regression analysis was used to pre-
dict the outcomes evaluated by the Stulberg classifica-
tion. The ordinal logistic regression analysis was utilized
for 294 of 304 patients who had data consisting of age
at diagnosis, sex, affected side, Herring classification
and the time of classification after onset, treatment
methods [operative methods: Salter innominate
osteotomy (SIO), femoral varus osteotomy (FVO);
conservative methods: bilateral abduction with full
weight-bearing (BFW), bilateral abduction with
non-weight-bearing (BNW), hemiabduction with full
weight-bearing (HFW), hemiabduction with partial
weight-bearing (HPW), and hemiabduction with
non-weight-bearing (HNW)], follow-up period, and
Stulberg evaluation. In the ordinal logistic regression
analysis, the Stulberg evaluation was set as a predictor
(dependent variable), and the other data were defined
as independent factors or covariates. The odds ratio was
expressed by a ordinal number as exp(B); for example,
for the risk ratio of sex (female/male: female as a
numerator and male as a denominator), exp(B)
=
1.5
means that females have a prognosis that is 1.5 times
worse than that of males. All statistical analyses were
conducted using the statistical package of Social Science
(SPSS) version 12.0J software. The critical values for
significance were set at P
<
0.05.
Results
Altogether, 95 institutions and hospitals, including all
of the children’s hospitals and university hospitals, en-
gaged in pediatric orthopedics in Japan responded to
the survey. There were a total of 711 patients with 766
affected hips. A total of 217 patients were affected in
1993, 266 in 1994, and 228 in 1995 (Table 1), with 606
male and 95 female patients. The average age at diagno-
sis was 7 years 1 month (2.3–14.3 years). A total of 281
right hips were affected, 372 left hips, and 55 cases of
both hips (7.7%). A total of 38 patients had associated
complications or disorders: 6 had hormonal disease (4
hypothalamic dwarfism, 2 hypothyroidism), 2 had short
status (
<
2 SD), 1 had scoliosis, 1 had hemihypertrophy,
3 had DDH, 1 had club foot, 1 had MED, 1 had a
habitual patellar dislocation, 13 had an allergic disorder,
3 had congenital heart disease, 2 had a genetic disorder,
1 had mental retardation, 1 had femoral lateral condylar
osteonecrosis, 1 had an auditory disorder, 1 had a
squint, and 1 infant had low body weight. Pain was the
chief problem in 92%, hip joint pain in 56%, knee joint
pain in 12.5%, thigh pain in 9.2% and no pain in 8%.
Gait pain (83.3%) and limping gait (96%) were also
symptoms (Table 2). There was a positive family history
in 4.5% of patients, with 50% of these patients having
an affected sibling (Table 3). There was a positive sports
history in 14.2% of the patients (Table 3).
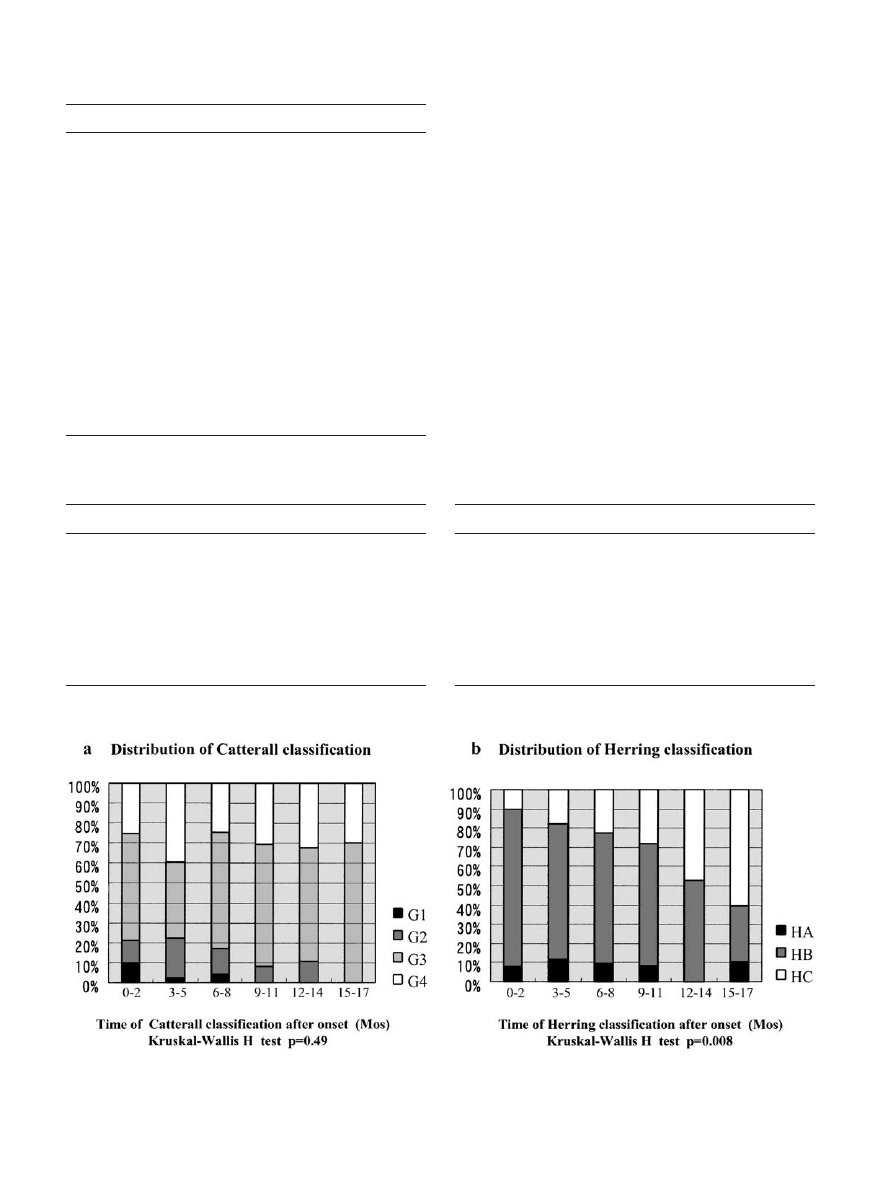
Using the Catterall classification, 50.6% of the pa-
tients were classified as group 3 and 30.2% as group 4
(Table 4). There was no significant correlation between
the distribution of the Catterall classification and the
time of classification after onset (Fig. 1a). In the Herring
Table 1. Incidence of LCPD from 1993 to 1995 in Japan
LCPD
Population (
<
15 ages)
Incidence (/10
5
)
Year
M/F/total
M/F/total (
×
10
6
)
M/F/total
1993
190/27/217
13.7/13.0/26.7
1.39/0.21/0.81
1994
230/36/266
13.5/12.3/25.8
1.70/0.29/1.03
1995
199/29/228
13.6/12.6/26.2
1.46/0.23/0.87
Average
1.51/0.24/0.90
LCPD, Legg-Calvé-Perthes disease; M, males; F, females
Table 2. Symptoms of LCPD
Symptom
No. of patients
No pain
58/695 (8%)
Pain
637/ 695 (92%)
Hip
359
Knee
80
Thigh
59
Hip and knee
44
Hip and thigh
42
Thigh and knee
15
Hip, thigh, and knee
11
Leg or foot
9
Others
8
Gait pain
443/532 (83.3%)
Limping gaits
626/652 (96.0%)
335
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
classification, 60.9% of patients were type B and 27.3%
type C (Table 4). There was a significant correlation
between the distribution by the Herring classification
and the time of classification after onset (Kruskal-
Wallis H test: P
=
0.008) (Fig. 1b). Containment therapy
(447 abduction bracing, 17 Salter innominate oste-
otomy, 74 femoral varus osteotomy, 3 triple osteotomy,
among others) was performed in 632 (92.5%) of the
684 responding cases. Noncontainment therapy (3 non-
weight-bearing methods, 11 no abduction bracing after
limb traction, 4 no abduction bracing after sling, 3
restriction of physical exercise, 5 femoral valgus oste-
otomy, 4 anterior rotational osteotomy of the femoral
neck, 1 Chiari osteotomy, 1 vascularized bone graft
after biopsy, 2 trochanteric advancement) was utilized
for 35 patients (5.1%). A total of 16 (2.3%) patients
were kept under observation only and did not receive
any treatment (Table 5).
To compare the outcomes, 304 of 611 patients who
had been evaluated by the Stulberg classification were
Table 4. Catterall and Herring classifications
Parameter
No.
Catterall classification
Group 1 (G1)
30 (4.3%)
Group 2 (G2)
103 (14.8%)
Group 3 (G3)
352 (50.6%)
Group 4 (G4)
210 (30.2%)
Herring classification
Type A (HA)
68 (11.8%)
Type B (HB)
350 (60.9%)
Type C (HC)
157 (27.3%)
Table 3. Family and sports history
Historical factor
No.
Family history
Negative
530 (95.5%)
Positive
25 (4.5%)
Siblings
12
Father
7
Others
2
No response
4
No response
10
Sports history
Not engaged
350 (85.8%)
Engaged
58 (14.2%)
Soccer
27
Baseball
10
Gymnastics
4
Field athletics
4
Swimming
3
Others
7
No response
2
No response
303
Fig. 1. a Catterall classification and the time of classification. b Herring classification and the time of classification
Table 5. Treatment methods for LCPD in Japan
Treatment
No.
Containment methods
632/683 (92.5%)
Conservative
519 (82.1%)
Operative
113 (17.9%)
Noncontainment methods
35/683 (5.1%)
Conservative
25 (71.4%)
Operative
10 (28.6%)
Observation
16/683 (2.3%)
No response
28
Total
711

336
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
selected; they had been classified when
>
13 years of age
or had been followed up for more than 3.5 years after
their diagnosis of LCPD. Of the 304 patients, 76 (25%)
were Stulberg type I, 135 (44%) were type II, 69 (23%)
were type III, 21 (7%) were type IV, and 3 (1%) were
type V (Table 6). Altogether, 96.7% of Herring type A
patients were Stulberg type I or II (100% of Catterall
group 1 and 93.5% of Catterall group 2). Therefore, to
compare the outcomes of the seven treatment methods,
Catterall groups 1 and 2 and Herring type A patients
were excluded from the younger-group and the older-
group analyses (Tables 7, 8). However, there was no
significant difference among the six treatment methods
(HFW was excluded because of the small number of
subjects) in either the younger group or older group in
the Kruskal-Wallis H test.
An ordinal logistic regression analysis showed that
the Herring classification was the highest predictor; the
odds ratios for A/C and B/C were 0.030 and 0.170,
respectively. The age at the time of diagnosis of LCPD
was the next predictor, with an odds ratio of 1.445 by 1
year. The right hip joint showed a worse prognosis than
the left hip joint, with an odds ratio of 1.577. There was
a significant difference between conservative treatment
methods and operative methods, with an odds ratio of
1.872 (Table 9). There was no significant correlation
with outcome among conservative treatment methods
(BFW, BNW, HFW, HPW, HNW) (Table 10). There
was also no significant difference in the outcomes be-
tween the SIO and FVO (Table 11).
Discussion
Epidemiological data
There has been no previous epidemiological study of
LCPD in Japan. The number of patients with LCPD in
1993 was 217 (190 boys, 27 girls), 266 (230 boys, 36 girls)
in 1994, and 228 (199 boys, 29 girls) in 1995. The popu-
lation of children
<
15 years of age was 26.7 million in
1993, 25.8 million in 1994, and 26.2 in 1995 from the
tables of trends in population by sex and age of the
Japanese National Government Survey; the incidence
of LCPD was 0.81/100 000 in 1993, 1.03/100 000 in 1994,
and 0.87/100 000 in 1995 (Table 1). The average annual
incidence of LCPD was 0.9/100 000. The number of
LCPD patients in Japan was less than that of white
children previously reported
4–7
(Table 12). The
incidence was dependent on gender, race, country, and
Table 6. Outcome of 304 patients evaluated by Stulberg classification who had been
classified when
>
13 years of age or followed up for
>
3.5 years after LCPD diagnosis
Parameter
No.
Stulberg evaluation: classification time after onset (months)
12.0
±
2.2
a
I
76 (25%)
b
II
69 (23%)
III
135 (44%)
IV
21 (7%)
V
3 (1%)
Subjects of unilateral LCPD
Age at diagnosis (years)
7.0
±
2.1
a
Sex (no. of patients)
Male
270
Female
34
Affected side (no. of patients)
Right
140
Left
164
Follow-up periods (years)
5.0
±
1.0
a
Radiographic classification
Catterall classification (time after onset, months)
6.9
±
4.2
a
I
10
c
II
39
III
164
IV
91
Herring classification (time after onset, months)
6.6
±
3.9
a
A
30
c
B
204
C
70
a
Average
±
SD
b
Number and percent of patients
c
Number of patients
337
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
Table 7.
Outcomes of patients
<
8 years old (minus patients of Catterall groups 1 and 2 and Herring type A) (
n
=
173)
Age
Sex
Side
CaT
Catterall
HeT
Herring
OpT
BrP
StT
Stulberg classification
FU
Outcome
(years)
a
(M/F)
(Rt/Lt)
(months)
a
III
IV
(months)
a
BC
(months)
a
(months)
a
(years)
a
II
I
III
IV
V
(years)
a
SIO (
n
=
9)
6.7
±
0.8
9/0
6/3
8.0
±
3.5
7
2
8.0
±
3.5
5
4
5.1
±
2.4
—
12.5
±
1.4
3
5
1
0
0
5.8
±
1.0
FVO (
n
=
24)
6.4
±
1.2
21/3
14/10
4.0
±
3.3
11
13
4.3
±
3.7
15
9
5.6
±
3.4
—
11.5
±
1.3
8
6
7
3
0
5.1
±
0.8
HNW (
n
=
40)
6.0
±
1.5
39/1
21/19
8.8
±
4.1
26
14
8.2
±
3.3
30
10
—
19.3
±
7.0
11.0
±
2.1
9
2
2
5
4
0
5.0
±
0.8
HPW (
n
=
12)
6.1
±
1.3
10/2
3/9
6.3
±
3.5
9
3
6.4
±
3.4
8
4
—
12.9
±
4.3
11.8
±
2.1
4
2
5
0
0
5.8
±
1.2
BNW (
n
=
59)
6.0
±
1.3
52/7
30/29
7.4
±
4.0
31
28
7.0
±
3.9
46
13
—
17.5
±
7.3
11.0
±
1.5
12
31
11
5
0
5.0
±
0.8
BFW (
n
=
29)
5.5
±
1.4
27/2
18/24
8.0
±
4.9
17
12
7.5
±
4.5
14
15
—
17.0
±
7.3
10.9
±
1.9
4
1
0
1
3
2
0
5.3
±
1.2
SIO, Salter innominate osteotomy; FVO, femoral varus osteotomy; HNW, hemi non-weight-bearing brace; HPW, hemi partial-weight-be
aring brace; HFW, hemi full-weight-bearing brace;
BNW, bilateral non-weight-bearing brace; BFW, bilateral full-weight-bearing brace; CaT, time of Catterall classification; HeT, t
ime of Herring classification; OpT, time of operation; BrP,
bracing periods; StT, time of Stulberg evaluation; FU, follow-up period
a
Results are the average
±
SD
NS, Kruskal-Wallis H test
Table 8.
Outcomes of LCPD patients
≥
8 years old (minus patients of Catterall groups 1 and 2 and Herring type A) (
n
=
65)
Age
Sex
Side
CaT
Catterall
HeT
Herring
OpT
BrP
StT
Stulberg classification
FU
Outcome
(years)
a
(M/F)
(Rt/Lt)
(months)
a
III
IV
(months)
a
BC
(months)
a
(months)
a
(years)
a
II
I
III
IV
V
(years)
a
SIO (
n
=
4)
10.0
±
1.8
3/1
1/3
12.0
±
3.7
3
1
12.0
±
3.7
2
2
4.3
±
1.3
—
15.0
±
1.7
0
1
2
0
0
4.8
±
0.7
FVO (
n
=
14)
9.8
±
1.1
13/1
5/9
4.3
±
3.7
11
3
4.4
±
3.7
12
2
4.3
±
3.3
—
14.5
±
1.5
3
7
2
1
1
4.7
±
0.7
HNW (
n
=
11)
9.6
±
1.2
10/1
4/7
7.5
±
3.4
9
2
7.5
±
3.0
10
1
—
24.4
±
10.8
14.5
±
1.8
1
3
4
1
2
4.8
±
0.9
HPW (
n
=
3)
9.1
±
1.2
3/0
1/2
7.7
±
1.5
2
1
12.0
±
3.6
1
2
—
15.7
±
5.1
13.9
±
1.1
0
0
2
1
0
4.8
±
1.4
BNW (
n
=
29)
9.4
±
1.6
26/3
11/18
6.9
±
4.0
21
8
6.6
±
3.7
27
2
—
16.2
±
5.5
14.0
±
1.8
1
1
6
1
0
2
0
4.6
±
0.8
BFW (
n
=
4)
9.7
±
1.5
4/0
2/2
7.5
±
3.3
3
1
6.5
±
1.7
2
2
—
12.3
±
1.7
15.0
±
2.2
0
2
1
1
0
5.4
±
1.0
a
Results are the average
±
SD
NS, Kruskal-Wallis H test
338
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
Table 11. Ordinal logistic regression analysis: operative cases (n
=
57)
95% CI for Exp(B)
Factor
B
SE
Wald
Lower
Exp(B)
Upper
Age at diagnosis (years)
0.350
0.150
5.467*
1.058
1.419
1.902
Sex (female/male)
0.134
0.883
0.023
0.202
1.144
6.458
Affected side (Rt/Lt)
−
0.033
0.507
0.004
0.358
0.967
2.614
Time of Herring evaluation (months)
−
0.034
0.089
1.073
0.921
1.096
1.304
Herring type
A/C
−
2.865
1.452
3.895*
0.003
0.057
0.980
B/C
−
1.497
0.691
4.694*
0.058
0.224
0.867
Treatment method (FVO/SIO)
0.806
0.727
1.227
0.538
2.238
9.313
Follow-up period (years)
0.205
0.272
0.645
0.730
1.245
2.123
Property of model: parallel line test: by the null hypothesis the
−
2 exponential likelihood is 132.097. By the general hypothesis it is 111.241
(
χ
2
=
20.838; df
=
24; P
=
0.648)
* P
<
0.05
Table 10. Ordinal logistic regression analysis: conservative cases (n
=
237)
95% CI for Exp(B)
Factor
B
SE
Wald
Lower
Exp(B)
Upper
Age at diagnosis (years)
0.389
0.067
34.02***
1.295
1.475
1.681
Sex (F/M)
0.307
0.401
0.588
0.620
1.360
2.983
Affected side (Rt/Lt)
0.590
0.262
5.071*
1.079
1.803
3.012
Time of Herring evaluation (months)
−
0.072
0.035
4.204
0.868
0.930
0.997
Herring type
A/C
−
3.623
0.587
38.12***
0.008
0.027
0.084
B/C
−
1.672
0.359
21.70***
0.093
0.188
0.380
Treatment method
BFW/HPF
0.800
0.538
2.215
0.779
2.226
6.386
BNW/HPF
0.449
0.505
0.791
0.582
1.567
4.220
HFW/HPF
−
0.856
0.945
0.819
0.067
0.425
2.711
HNW/HPF
0.425
0.543
0.612
0.528
1.530
4.434
Bracing periods (months)
0.028
0.020
1.949
0.989
1.028
1.069
Follow-up period (years)
0.209
0.137
2.335
0.943
1.233
1.613
Property of model (paralell line test): by the null hypothesis the
−
2 exponential likelihood is 507.902. By the general hypothesis, the
−
2
exponential likelihood is 490.026 (
χ
2
=
17.873; df
=
36; P
=
0.995)
* P
<
0.05; ** P
<
0.01; *** P
<
0.001
Table 9. Ordinal logistic regression analysis: all cases (n
=
294)
95% CI for Exp(B)
Factor
B
SE
Wald
Lower
Exp(B)
Upper
Age at diagnosis (years)
0.368
0.059
39.23***
1.288
1.445
1.621
Sex (female/male)
0.282
0.355
0.628
0.661
1.325
2.658
Affected side (Rt/Lt)
0.455
0.226
4.071*
1.013
1.577
2.454
Time of Herring evaluation (months)
−
0.034
0.031
1.202
0.910
0.967
1.027
Herring type
A/C
−
3.498
0.526
44.30***
0.011
0.030
0.085
B/C
−
1.774
0.305
33.74***
0.093
0.170
0.309
Treatment method Con/Ope
0.627
0.296
4.502*
1.049
1.872
3.341
Follow-up period (years)
0.205
0.119
2.971
0.972
1.228
1.550
Property of model (parallel line test): by the null hypothesis the
−
2 exponential likelihood is 651.788. By the general hypothesis, the
−
2
exponential likelihood is 640.648 (
χ
2
=
11.140; df
=
24; P
=
0.988)
SE, standard error; 95% CI, 95% of confidence interval; Exp(B), exponential B
=
Odds ratio
* P
<
0.05; ** P
<
0.01; *** P
<
0.001

339
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
Table 12. Incidence of LCPD
Incidence
Year
Study
Location
Males
Females
Total (/10
5
)
1966
Molloy
4
Massachusetts, USA
0.57
1972
Gray
5
British Columbia, Canada
8.4
1.6
5.1
1983
Hall
6
Liverpool, England
25.8
4.9
15.6
1992
Moberg
7
Uppsala, Sweden
8.5
2.1
6.3
2005
Multicenter study in Japan
1.51
0.24
0.9
economic situation.
6
As for incidence, the white races
had a higher incidence than the yellow races, and the
yellow races were higher than the black races.
6
Bilateral
hips were affected in 7.7% of this series. In 1978,
Wynne-Davies and Gormley
8
reported the incidence of
bilateral LCPD to be 11.3% among Edinburgh and
Glasgow patients. If the research period had been
longer than 3 years, the incidence of bilateral LCPD
might have increased.
The symptoms of LCPD were pain, gait pain, and
limping gait. Pain located only in the hip joint was re-
ported in 56.4% of patients, only in the knee joint in
12.5%, and only in the thigh in 9%. In total, 92.0% of
patients complained of pain, with 8% having no pain.
Special attention should be paid to the group of patients
who did not have any pain at the time of the initial
consultation (Table 2). Patients with a history of gait
pain comprised 83.3% of the total number, and 96.0%
of the patients had a history of limping gait.
The genetic problems described were also found in
siblings, twins, cousins, father, or uncles with skeletal
problems. Wynne-Davies and Gormley
8
reported an
incidence of LCPD of 1.0% among first-degree rela-
tives, 0.3% among second-degree relatives, and 0.3%
among third-degree relatives. The family history was
positive in 4.5% of this series. It was thought that a
lower incidence of a positive family history as well as the
incidence of LCPD depended on the factor of race
(Asian people).
Herring type B was a major type of radiographic
classification, accounting for more than 60% in this
series. Recently, Herring et al.
9
tried to use type B/C a
modified lateral pillar classification to provide a more
precise classification for prognostic evaluation. We
could not use the modified lateral pillar classification in
this study because the study started prior to Herring
et al.’s report. The optimal time for applying the Her-
ring classification was more than 7 months after the
onset because the decreasing rate of lateral pillar height
plateaued 7 months later.
10
However, the distribution
of Herring types significantly depended on the time
of classification after onset of LCPD in this study
(Kruskal-Wallis H test: P
=
0.008) (Fig. 1b). This was
reasonable because the Herring types indicated that the
height of the lateral pillar had gradually decreased
with time after the onset of LCPD. The Catterall
classification had no significant correlation between the
Catterall groups and the time of classification after the
onset of LCPD because there was change in the necrotic
area, which does not depend on the time after onset
(Fig. 1a). However, the Catterall classification was
difficult to perform because it requires two-plane radio-
graphic assessment, which had been changed by the
deformity of the residual bone.
Treatment methods in Japan
Since Legg, Calvé, and Perthes first described the
pathological condition of LCPD in 1910, the main treat-
ment methods have been long bed rest and traction
of the affected limb, as reported by Danforth
11
and
Sundt.
12
There were many problems associated with
prolonged bed rest, and hence ambulatory treatments
using a non-weight-bearing technique were applied. In
1958, Evans and Lloyd-Roberts
13
reported that the out-
come of the Snyder
14
sling for LCPD was the same as
that of bed rest. In 1966, Harrison
15
reported the useful-
ness of containment methods that had been previously
advocated by Parker in 1929. The use of containment
methods then spread throughout the world. In Japan,
many treatment methods have been applied for LCPD,
including bilateral abduction casts or a brace, using
bilateral abduction braces such as the Newington
brace,
16
the Atlanta brace (Scottish-Rite),
17
the Bach-
elor (Toronto), and the modified abduction cast
(A-cast).
18–20
However, all of these patients were forced
into long periods of hospitalization in institutions.
Nowadays, many ambulatory orthoses for outpatients
have been tried. Patients with these braces are able to
go to school and attend the hospital as outpatients only.
Of this group, the Tachdjian brace,
21
the Nishino abduc-
tion brace,
22
the modified pogo-stick brace,
23,24
and the
SPOC (Shiga Pediatric Orthopaedic Centre) brace
25
are
currently popular in Japan. However, noncontainment
methods such as traction, non-weight-bearing, and
prolonged bed rest are still in use in some institutions.
Operative methods include varus osteotomy, Salter in-
nominate osteotomy, triple osteotomy, femoral valgus

340
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
osteotomy, femoral neck rotational osteotomy, Chiari
osteotomy, vascularized bone graft, and great tro-
chanteric advancement. A total of 519 (82.1%) of 632
patients with LCPD were treated by conservative con-
tainment methods (HFW, HPW, HNW, BFW, BNW),
and 113 (17.9%) of 632 patients with LCPD were
treated by operative containment methods (SIO and
FVO) during this period in Japan.
Treatment methods and outcomes of unilateral LCPD
In 1986, Cooperman and Stulberg
26
reported the out-
comes of 248 cases treated by non-weight-bearing with
crutches, an Atlanta brace, a Newington abduction or-
thosis, and varus osteotomy of the femur. Stulberg types
I and II accounted for 50% of the non-weight-bearing
patient group, 64% of the Atlanta brace group, 71% of
the Newington abduction orthosis group, and 70% for
the varus osteotomy group. In 1995, Wang et al.
27
re-
ported that “good” and “fair” outcomes, as evaluated
by Mose’s
28
methods, were found in 49% of non-weight-
bearing with physical exercise patients, 49% of Atlanta
brace patients, 62% of Petrie cast patients 60% of varus
osteotomy patients, and 60% of Salter innominate
osteotomy patients.
18
A study by Grzegorzewski et al.
29
analyzed 142 cases, of which Stulberg types I and II
comprised 61 (80%) of 76 of the long-term rest and limb
traction management group, 15 (71%) of 21 of the
Petrie cast group, 53 (74%) of 74 the abduction orthosis
group, and 19 (73%) of 26 in the varus osteotomy
group. Grzegorzewski et al. reported that no significant
difference was found among the groups.
All of these studies concluded that there was no
significant difference in outcome among the treatment
methods for LCPD. The studies, however, cited many
factors related to the outcomes of LCPD. Herring et al.
noted that the lateral pillar classification and the age at
the onset of LCPD were highly and strongly correlated
with the outcomes evaluated by the Stulberg classifica-
tion.
30
Therefore, in this study the subjects were divided
into a young group and an older group to avoid the age
effect on the outcomes of the seven treatment methods.
In the
<
8 years old group, Stulberg type I and II ac-
counted for 8 (89%) of 9 patients treated by SIO, 14
(58%) of 24 patients treated by FVO, 31 (78%) of 40
patients treated by HNW (modified pogo-stick, Nishio,
Tachdjian), 6 (55%) of 11 patients treated by HPW
(SPOC), 43 (73%) of 59 patients treated by BNW (A-
cast, modified A-cast, Bachelor brace), and 14 (48%) of
29 patients treated by BFW (Toronto, Atlanta, A-cast
brace) (Table 7). In the
≥
8 years old group, Stulberg
types I and II accounted for 1 (33%) of 3 patients
treated by SIO, 10 (71%) of 14 patients treated by FVO,
4 (36%) of 11 patients treated by HNW, 0 of 3 patients
treated by HPW, 17 (59%) of 29 patients treated by
BNW, and 2 (50%) of 4 patients treated by BFW (Table
8). In the
<
8 years old group, SIO, HNW, and BNW had
good outcomes compared to other treatment methods
(Table 7). In the older group, FVO had the best out-
come compared to other treatment methods (Table 8).
For the older patients FVO showed better outcome
than SIO, and SIO seemed to have better outcome than
FVO in the young group. It was thought that SIO had
better coverage of the femoral head in the young group
than in the older group. However, there was no signifi-
cant difference between SIO and FVO because of the
small numbers in each group (Kruskal-Wallis H test).
Odds ratios by ordinal logistic regression for
unilateral LCPD
Many factors have been thought to relate to the progno-
sis of LCPD. The ordinal logistic regression analysis
showed that Herring classification, age at diagnosis, and
the side affected were significantly correlated with the
outcome (Table 9). It had not been reported previously
that the left hip joint in LCPD had a better prognosis
than the right hip joint. It is possible that the dominant
side of the lower extremity affected the outcome.
The operative methods (SIO and FVO) for LCPD gave
a significantly better prognosis than the conservative
methods (BFW, BNW, HFW, HPW, HNW), with an
odds ratio of 1.87 (P
=
0.034). However, with con-
servative treatment, there was no significant correlation
among the five treatment methods (Table 10). For
operative treatment, there was no significant difference
between SIO and FVO (Table 11). It was thought that
a larger number of subjects in each treatment group
is required for statistical significance. Many contain-
ment methods for LCPD have been performed in
Japan, and the optimal treatment method for LCPD
could not be determined in this study. The overall out-
come, however, was not worse than has been reported
worldwide.
Limitation of this study
In this series, we were unable to obtain the radiographic
assessment or the bone age at the time of LCPD diagno-
sis; nor did we have data on treatment delay, which
might affect the outcome. About one-third of the pa-
tients were skeletally mature at the time of the Stulberg
evaluation. Therefore, the outcomes of this series might
change after several years, and for this reason the pa-
tients should be followed up in the next multicenter
study for LCPD.
Acknowledgments. The members of the MCS committee of
JPOA thank the 95 children’s hospitals and institutions in
Japan for their collaboration.

341
W.-C. Kim et al.: Multicenter study of Legg-Calvé-Perthes disease
References
1. Catterall A. The natural history of Perthes’ disease. J Bone Joint
Surg Br 1971;53:37–53.
2. Herring JA, Neustadt JB, Williams JJ, Early JS, Browne RH.
The lateral pillar classification of Legg-Calvé-Perthes disease, J
Pediatr Orthop 1992;12:143–50.
3. Stulberg SD, Cooperman DR, Wallensten R. The natural history
of Legg-Calvé-Perthes disease. J Bone Joint Surg Am 1981;63:
1095–108.
4. Molloy MK, MacMahon B. Incidence of Legg-Perthes disease
(osteochondritis deformance). N Engl J Med 1966;275:988–90.
5. Gray IM, Lowry RB, Renwick DH. Incidence and genetics of
Legg-Perthes disease (osteochondritis deformans) in British
Columbia: evidence of polygenic determination. J Med Genet
1972;9:197–202.
6. Hall AJ, Barker DJ, Dangerfield PH, Taylor JF. Perthes’ disease
of the hip in Liverpool. BMJ 1983;287:1757–9.
7. Moberg A, Rehnberg L. Incidence of Perthes’ disease in Uppsala,
Sweden. Acta Orthop Scand 1992;63:157–8.
8. Wynne-Davies R, Gormley J. The aetiology of Perthes’ disease:
genetic, epidemiological and growth factors in Edinburgh and
Glasgow patients. J Bone Joint Surg Br 1978;60:6–13.
9. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease,
Part I. Classification of radiographs with use of the modified
lateral pillar and Stulberg classifications. J Bone Joint Surg Am
2004;86:2103–18.
10. Lappin K, Kealey D, Cosgrove A. Herring classification: how
useful is the initial radiograph? J Pediatr Orthop 2002;22:479–82.
11. Danforth M. The treatment of Legg-Calvé-Perthes disease. J
Bone Joint Surg 1934;16:516–34.
12. Sundt H. Further investigation respecting mature coxae: Calvé-
Legg-Perthes disease with special regard to prognosis and treat-
ment. Acta Chir Scand Suppl 1949;148:1–101.
13. Evans DL, Lloyd-Roberts GC. Treatment in Legg-Calvé-Perthes’
disease: a comparison of in-patient and out-patient methods. J
Bone Joint Surg Br 1958;40:182–9.
14. Snyder CH. A sling for use in Legg-Perthes disease. J Bone Joint
Surg 1947;29:524–6.
15. Harrison MHM. Legg-Calvé-Perthes disease: the value of
roentgenographic measurement in clinical practice with special
reference to the Broomstick plaster method. J Bone Joint Surg
Am 1966;48:1301–18.
16. Martinez AG, Weinstein SL, Dietz FR. The weight-bearing ab-
duction brace for the treatment of Legg-Perthes disease. J Bone
Joint Surg Am 1992;74:12–21.
17. Meehan PL, Angel D, Nelson JM. The Scottish Rite abduction
orthosis for the treatment of Legg-Perthes disease: a radiographic
analysis. J Bone Joint Surg Am 1992;74:2–12.
18. Petrie JG, Bitenc I. The abduction weight-bearing treatment in
Legg-Calvé-Perthes’ disease. J Bone Joint Surg Br 1971;53:54–62.
19. Tamura K, Inoue N, Ishioka T. Evaluation of modified A-cast in
the treatment of Legg-Calvé-Perthes’ disease. J Joint Surg 1985;4:
257–63 (in Japanese).
20. Tamura K, Futami T, Kobayasi M, Akiyama N. Long-term results
and its limitations of modified Petrie’ s cast. J Jpn Paediatr Orthop
Assoc 1993;3:157–62 (in Japanese).
21. Tachdjian MO, Jouett LD. Trilateral socket hip abduction
orthosis for the treatment of Legg-Perthes’ disease. Orthosis
Prosthetics 1968;22:49–62.
22. Kubota H, Noguchi Y, Nakashima Y, Suenaga E, Iwamoto Y.
Long-term follow up of conservative treatment (Nishio’s brace)
of Perthes’ disease. J Jpn Paediatr Orthop Assoc 2000;9:15–8 (in
Japanese).
23. Kim W-C, Kubo T, Hirasawa Y, Kusakabe T. Comparison be-
tween Tachdjian brace and modified pogo-stick brace for Perthes’
disease using Gait analysis. J Jpn Paediatr Orthop Assoc 1995;4:
275–9 (in Japanese).
24. Kim W-C, Hosokawa M, Tsuchida Y, Kawamoto K, Kubu T,
Hirasawa Y, et al. Outcome of conservative treatment with new
pogo-stick brace for unilateral Perthes’ disease. J Jpn Paediatr
Orthop Assoc 2000;9:85–8 (in Japanese).
25. Kasahara Y, Seto Y, Ohura K. Conservative treatment of Legg-
Calvé-Perthes disease with SPOC-brace and its restration pattern
of the affected femoral head. J Joint Surg 1986;5:93–104 (in
Japanese).
26. Cooperman DR, Stulberg SD. Ambulatory containment treat-
ment in Perthes’ disease. Clin Orthop 1986;203:289–00.
27. Wang L, Bowen JR, Puniak MA, Guille JT, Glutting J. An evalu-
ation of various methods of treatment of Legg-Calvé-Perthes
disease. Clin Orthop 1995;314:225–33.
28. Mose K. Methods of measuring in Legg-Calvé-Perthes disease
with special regard to the prognosis. Clin Orthop 1980;150:103–9.
29. Grzegorzewski A, Bowen JR, Guille JT, Glutting J. Treatment of
the collapsed femoral head by containment in Legg-Calvé-
Perthes disease. J Pediatr Orthop 2003;23:15–9.
30. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease.
Part II. Prospective multicenter study of the effect of treatment on
outcome. J Bone Joint Surg Am 2004;86:2121–34.
Wyszukiwarka
Podobne podstrony:
Legg Calvé Perthes Disease in Czech Archaeological Material
A recurrent mutation in type II collagen gene causes Legg Calvé Perthes disease in a Japanese family
Intertrochanteric osteotomy in young adults for sequelae of Legg Calvé Perthes’ disease—a long term
Femoral head vascularisation in Legg Calvé Perthes disease comparison of dynamic gadolinium enhanced
Legg Calvé Perthes disease multipositional power Doppler sonography of the proximal femoral vascular
Acute chondrolysis complicating Legg Calvé Perthes disease
Modified epiphyseal index for MRI in Legg Calve Perthes disease (LCPD)
Legg Perthes disease in three siblings, two heterozygous and one homozygous for the factor V Leiden
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Dynamic gadolinium enhanced subtraction MR imaging – a simple technique for the early diagnosis of L
Hip Arthroscopy in Legg Calve Perthes Disease
Computerized gait analysis in Legg Calve´ Perthes disease—Analysis of the frontal plane
Coxa magna quantification using MRI in Legg Calve Perthes disease
Osteochondritis dissecans in association with legg calve perthes disease
Interruption of the blood supply of femoral head an experimental study on the pathogenesis of Legg C
Legg Calve Perthes’ disease
Legg Calve Perthes’ disease
Legg Calve Perthes disease The prognostic significance of the subchondral fracture and a two group c
więcej podobnych podstron