Contents
lists
available
at
Resuscitation
j o
u
r n
a l
h o m
e p a g e
:
w w w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Commentary
and
concepts
Guidance
for
ambulance
personnel
on
decisions
and
situations
related
to
out-of-hospital
CPR
夽
Anders
Ågård
,
Johan
Herlitz
,
Maaret
Castrén
,
Lars
Jonsson
,
Lars
Sandman
a
Sahlgrenska
Academy,
Institute
of
Medicine,
Gothenburg,
Sweden
b
The
Center
for
Prehospital
Research
in
Western
Sweden,
University
College
of
Borås
and
Sahlgrenska
University
Hospital,
Gothenburg,
Sweden
c
Department
of
Clinical
Science
and
Education,
Karolinska
Institutet,
Södersjukhuset,
Stockholm,
Sweden
d
Stockholm
Prehospital
Centre,
Södersjukhuset,
Stockholm,
Sweden
e
School
of
Health
Science,
University
of
Borås,
Sweden
a
r
t
i
c
l
e
i
n
f
o
Article
history:
Received
15
March
2011
Received
in
revised
form
15
July
2011
Accepted
20
July
2011
Keywords:
Cardiopulmonary
resuscitation
Prehospital
emergency
care
Ethics
Practice
guideline
Ambulance
a
b
s
t
r
a
c
t
Ethical
guidelines
on
out-of-hospital
cardio-pulmonary
resuscitation
(CPR)
are
designed
to
provide
sub-
stantial
guidance
for
the
people
who
have
to
make
decisions
and
deal
with
situations
in
the
real
world.
The
crucial
question
is
whether
it
is
possible
to
formulate
practical
guidelines
that
will
make
things
some-
what
easier
for
ambulance
personnel.
The
aims
of
this
article
are
to
address
the
ethical
aspects
related
to
out-of-hospital
CPR,
primarily
to
decisions
on
not
starting
or
terminating
resuscitation
attempts,
using
the
views
and
experience
of
ambulance
personnel
as
a
starting
point,
and
to
summarise
the
key
points
in
a
practice
guideline
on
the
subject.
© 2011 Elsevier Ireland Ltd. All rights reserved.
1.
Introduction
The
rationale
for
guidelines
including
the
ethics
of
resuscitation
is
to
enable
professionals
to
make
more
appropriate
decisions
and
to
act
more
effectively
compared
with
what
might
happen
if
their
decisions
and
actions
were
only
based
on
individual
judgements
and
their
own
values.
challenge
is
to
provide
substantial
guidance
on
questions
or
problems
that
are
experienced
in
the
real
world.
Ambulance
personnel
are
confronted
by
a
number
of
ethical
considerations
when
they
are
on
their
way
to
treat
a
person
who
has
suffered
an
out-of-hospital
cardiac
arrest
(OHCA)
with
car-
diopulmonary
resuscitation
most
crucial
question
is
whether,
and
in
which
particular
circumstances,
they
can
be
given
a
mandate
to
decide
to
terminate
a
resuscitation
attempt
at
the
scene.
The
aims
of
this
article
are
to
address
and
to
clarify
the
ethi-
cal
aspects
related
to
out-of-hospital
CPR,
based
on
our
knowledge
夽 A
Spanish
translated
version
of
the
abstract
of
this
article
appears
as
Appendix
in
the
final
online
version
at
doi:10.1016/j.resuscitation.2011.07.028
.
∗ Corresponding
author
at:
Medicinmottagningen,
Angereds
Närsjukhus,
Box
22,
SE-424
65
Göteborg,
Sweden.
Tel.:
+46
31
3326700;
fax:
+46
31
3320369;
mobile
+46
0
761
360364.
address:
(A.
Ågård).
of
the
views
and
experience
of
ambulance
personnel,
and
to
summarise
the
key
points
in
a
practice
guideline
on
the
sub-
ject.
2.
The
objective
of
CPR
From
the
ambulance
personnel’s
point
of
view,
a
reasonable
way
to
measure
the
effectiveness
of
a
resuscitation
attempt
is
whether
patients
affected
by
an
OHCA
have
spontaneous
circulation
when
they
are
delivered
to
the
emergency
room.
this
way
of
defining
what
constitutes
successful
CPR
hardly
applies
from
the
patient’s
viewpoint.
We
argue
that
the
objective
of
CPR
is
to
restore
life
with
quality
acceptable
to
the
patient
and
in
accordance
with
his
or
her
will.
To
properly
evaluate
the
effectiveness
of
their
attempts,
personnel
involved
in
out-of-hospital
CPR
must
therefore
be
informed
about
the
outcome
of
the
patients
in
a
systematic
quality
improvement
system.
In
some
ambulance
systems,
they
are
only
aware
of
and
are
only
evaluated
on
the
basis
of
prehospital
results.
3.
Choices
to
be
made
When
confronted
by
a
person
with
cardiac
arrest,
the
emer-
gency
personnel
can
initiate
and
then
continue
CPR,
or
initiate
and
subsequently
stop
CPR
or
withhold
CPR
in
the
first
place.
If
CPR
is
0300-9572/$
–
see
front
matter ©
2011 Elsevier Ireland Ltd. All rights reserved.
doi:
28
A.
Ågård
et
al.
/
Resuscitation
83 (2012) 27–
31
Algorithm for the treatment of an out-of-hospital cardiac arrest
Obvious evidence of
irreversible death
do-not-attempt-resuscitation
(DNAR)
mortis, deco
DNAR
Stop
resuscitation
attempt
No
Start CPR
Connect defibrillator
ECG analysis
Defibrillate?
No
Yes
Yes
No/Unknown
Yes
CPR according
to guidelines
Yes
Cardiac
arrest
Continued asystole during
> 20 min
CPR
If suspected:
Drowning
Hypothermia
Intoxication
Obvious
pregnancy
Continued effective CPR
Transport to hospital
–
–
–
–
Asystole
Not witnessed
No bystander CPR
Alarm –
arrival
>15 min
(the decision takes account of the
patient’s biological age)
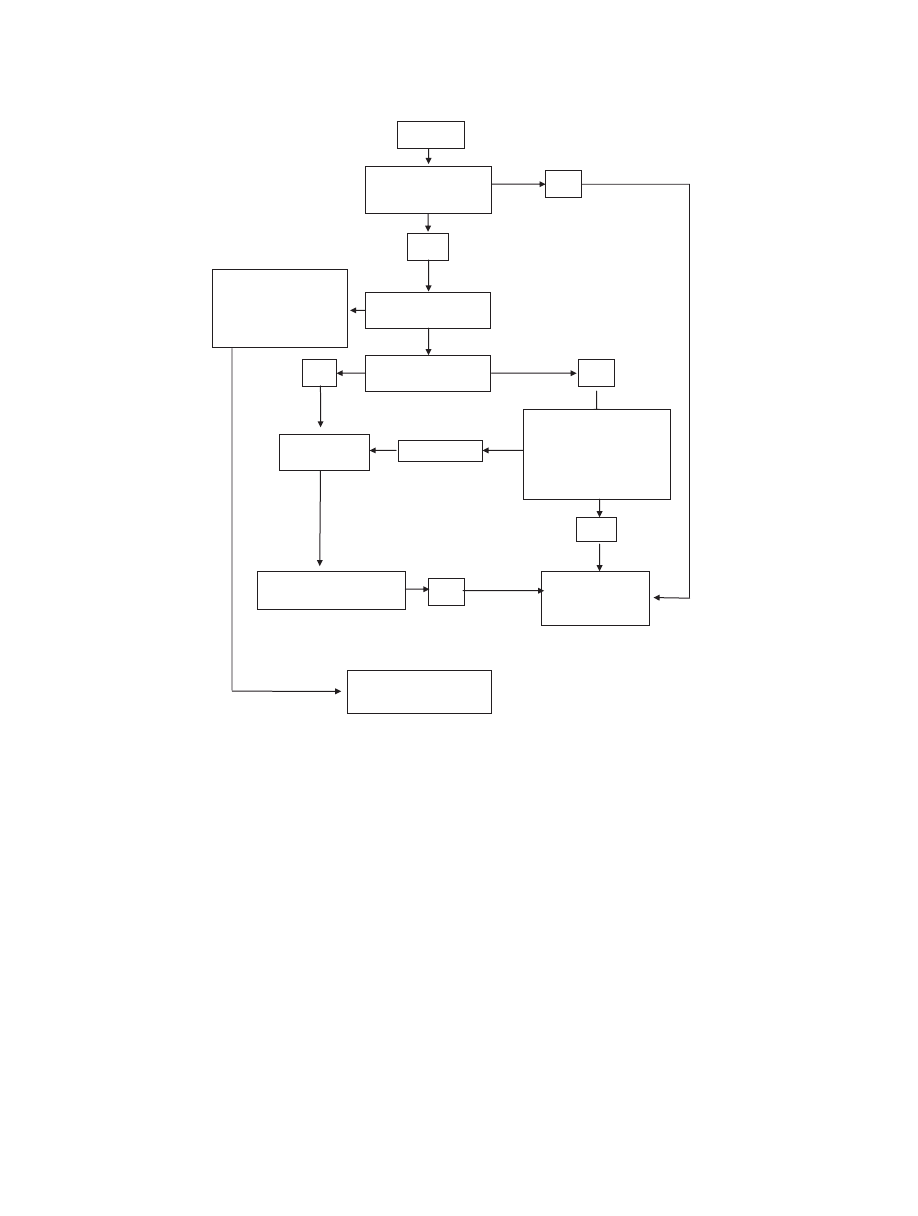
Fig.
1.
Algorithm
for
the
treatment
of
an
out-of-hospital
cardiac
arrest.
initiated,
the
patient
has
a
chance
to
be
saved
for
a
life
of
acceptable
quality
or
a
life
with
less
than
acceptable
quality.
If
CPR
is
withheld,
the
patient
will
definitely
die.
There
are
strong
reasons
for
ambulance
personnel
to
initiate
CPR
routinely
on
persons
who
have
suffered
an
OCHA.
Firstly,
the
infor-
mation
about
the
patient’s
medical
condition
before
the
cardiac
arrest
is
often
insufficient.
Second,
the
patient’s
preference
regard-
ing
CPR
is
generally
unknown.
Third,
it
is
difficult
to
make
correct
prognoses
about
the
chances
of
survival
and
quality
of
life
following
resuscitation
attempts.
However,
there
are
reasonable
exceptions
to
the
general
rule
to
initiate
CPR,
such
as
cases
of
obvious
mortal
injury
or
death.
Moreover,
taking
the
available
knowledge
relating
to
factors
that
influence
the
outcome,
clinical
prediction
rules
and
algorithms
for
terminating
resuscitative
efforts
in
the
field
have
been
proposed.
We
suggest
an
alternative
algorithm
for
the
treatment
of
an
OHCA
that
includes
criteria
for
stopping
resuscitation
attempts
By
looking
retrospectively
at
the
records
from
the
Swedish
Cardiac
Arrest
Registry,
we
calculate
that
CPR
would
be
stopped
after
a
short
period
in
approximately
2%
of
the
cases
if
the
algorithm
were
implemented
in
our
services.
The
registry
does
not
include
patients
on
whom
CPR
was
not
initiated
because
of
obvious
death
signs
or
ethical
reasons.
4.
Attempting
to
act
in
the
patient’s
best
interest
CPR
is
sometimes
considered
futile
or
unethical,
even
in
cases
where
there
is
a
small
chance
of
saving
lives.
Among
patients
affected
by
severe
diseases,
which
substantially
influence
their
quality
of
life
and
expected
remaining
lifetime,
doubts
can
be
raised
about
whether
CPR
is
in
the
patient’s
best
interest.
Studies
have
actually
shown
that
the
ambulance
personnel
sometimes
drive
more
slowly
than
normal
to
the
scene
when
the
emergency
call
relates
to
a
very
old,
very
ill
patient
with
a
cardiac
arrest.
They
may
occasionally
feel
that
prehospital
resources
are
not
used
cost
effec-
tively.
Moreover,
they
may
not
try
as
hard
as
they
normally
do
to
optimise
the
CPR
procedure
in
this
category
of
patients.
A
com-
mon
argument
for
this
behaviour
is
their
wish
not
to
take
away
a
peaceful,
dignified
death
from
the
patient
and
family.
ever,
references
to
‘dignity’
are
problematic.
In
fact,
the
concept
of
a
dignified
death
can
be
interpreted
in
a
number
of
different
ways.

A.
Ågård
et
al.
/
Resuscitation
83 (2012) 27–
31
29
Studies
have
shown
that
patients
in
the
late
stages
of
chronic
diseases
may
want
CPR
to
be
given
the
chance
to
live
a
little
even
though
the
prognosis
is
statistically
poor
and
the
chronological
age
is
high,
patients
may
benefit
from
CPR
and
regain
an
acceptable
quality
of
life.
As
a
result,
it
is
generally
beyond
the
competence
of
the
emergency
personnel
to
assess
whether
or
not
a
resuscitation
attempt
is
in
the
patient’s
best
interest,
or
to
determine
the
kind
of
death
the
patient
would
have
preferred.
Being
in
the
presence
of
a
person
with
cardiac
arrest,
hav-
ing
first-hand
information
and
being
able
to
make
an
appropriate
examination
is
a
great
advantage.
We
argue,
based
on
our
own
and
others’
experience,
that
emergency
services
staff
members
with
the
appropriate
training
could
be
given
a
mandate
to
decide
not
to
initiate
or
to
stop
a
resuscitation
attempt
under
well-defined
conditions.
the
same
time,
the
creation
of
an
organisation
in
which
emergency
personnel
can
easily
consult
physicians,
emer-
gency
doctors,
cardiologists
or
anaesthesiologists
at
the
prehospital
stage,
to
obtain
support
or
advice,
can
be
recommended.
An
organ-
isation
of
this
kind
has,
for
example,
been
created
in
Helsinki
and
Oslo.
5.
Advance
directives
In
principle,
there
are
two
ways
to
find
out
what
a
patient
would
have
wanted
in
the
event
of
an
OHCA.
Firstly,
if
possible
and
appro-
priate,
people
who
are
close
to
the
patient
could
be
asked
tactfully
what
they
think
the
patient
would
have
wanted
in
terms
of
CPR.
However,
this
does
not
mean
that
decisions
relating
to
out-of-
hospital
CPR
should
be
handed
over
to
them.
It
can
actually
be
a
burden
to
feel
responsible
for
making
a
decision
relating
to
life
and
death,
which
can
in
turn
give
rise
to
future
guilt
and
doubts,
for
example.
When
consulting
family
members,
it
should
be
remem-
bered
that
their
will
might
differ
from
the
will
of
the
patient
or
that
they
could
have
misinterpreted
the
patient’s
wishes.
As
a
result,
it
may
be
difficult
to
distinguish
between
what
is
in
the
patient’s
best
interest
and
the
family’s
best
interest.
Second,
this
is
possible
by
having
access
to
written
advance
directives.
The
whole
idea
of
documents
containing
advance
direc-
tives
is
to
give
people
a
chance
to
convey
their
wishes
or
exercise
their
autonomy,
in
situations
in
which
they
have
temporarily
or
permanently
lost
the
ability
to
do
this.
However,
there
are
ques-
tions
and
problems
related
to
the
legal
status
and
validity
of
these
documents.
For
instance,
even
if
the
advance
directives
state
that
a
person
does
not
want
CPR,
can
the
emergency
team
take
it
for
granted
that
the
document
belongs
to
the
person
with
a
cardiac
arrest
in
front
of
them,
that
the
patient
really
wanted
to
have
this
statement
written
down
and
that
the
person
has
not
changed
his
or
her
attitude
towards
CPR
since
then?
As
a
result,
emergency
personnel
should
be
recommended
to
deal
with
advance
direc-
tives,
such
as
do-not-resuscitate
orders,
critically
and
with
sound
judgement.
these
directives
should
generally
be
seen
as
a
valuable
help
when
attempting
to
make
a
decision
that
is
in
the
patient’s
best
interest.
6.
Withholding
or
withdrawing
CPR
Health
professionals
often
find
it
psychologically
more
difficult
to
withdraw
CPR
rather
than
not
starting
it
in
the
first
place.
a
result,
there
might
be
occasions
on
which
members
of
emergency
teams
are
unwilling
to
start
CPR
to
avoid
finding
themselves
in
a
situation
in
which
they
have
to
make
a
decision
to
terminate
the
treatment,
especially
in
the
presence
of
other
people.
In
our
opinion,
there
is
no
relevant
ethical
difference
between
not
initi-
ating
and
initiating
and
subsequently
withdrawing
CPR
from
the
patient’s
perspective,
as
the
consequence
is
basically
the
same
–
the
patient
will
die.
On
the
other
hand,
four
‘psychological’
reasons
for
continu-
ing
CPR
deemed
to
be
unsuccessful
or
futile
have
been
identified.
Firstly,
emergency
personnel
may
be
inclined
to
prolong
CPR
to
show,
or
convince,
those
around
them
that
“everything
that
can
possibly
be
done
is
actually
being
done.”
It
has
been
argued,
when
referring
to
the
potential
benefit
for
family
members,
that
this
way
of
acting
is
ethically
the
personnel
may
want
to
confirm
that
bystanders
did
the
right
thing
when
they
initiated
the
treatment.
the
personnel
want
to
escape
from
taking
care
of
grieving
persons,
who
just
have
lost
a
loved
one.
By
contin-
uing
CPR,
it
is
possible
to
transport
patients
to
hospital
who
have
not
yet
been
pronounced
dead.
Moreover,
some
members
of
the
emergency
team
may
not
even
feel
that
it
is
their
job
or
profes-
sional
responsibility
to
provide
emotional
support
at
the
scene.
Fourthly,
family
members
do
not
want
the
resuscitation
attempt
to
be
terminated.
We
argue
that
CPR
could
be
continued
for
a
short
period
of
time,
if
there
are
no
clear
signs
of
death,
even
though
it
may
be
deemed
not
to
be
successful,
to
assure
close
relatives
and
bystanders
that
everything
possible
has
been
done
and
that
their
efforts
were
com-
mendable.
Perhaps
this
strategy
could
also
ease
the
possible
guilt
of
not
being
successful
in
terms
of
restoring
the
function
of
the
heart.
The
persons
who
are
concerned
should
then
be
informed
clearly
and
tactfully
about
the
reasons
for
terminating
the
resuscitation
attempt.
7.
The
presence
of
family
members
and
bystanders
Despite
the
fact
that
life
or
death
is
at
stake
and
that
CPR
may
be
regarded
as
a
somewhat
violent
procedure,
most
people
want
to
be
near
their
loved
ones
during
resuscitation
some
members
of
the
emergency
team
may
feel
that
the
presence
of
per-
sons
close
to
the
patient
and
bystanders
constitutes
a
problem.
For
instance,
there
are
concerns
about
how
they
will
experience
wit-
nessing
a
resuscitation
attempt.
Emergency
personnel
may
also
feel
that
their
ability
to
provide
adequate
CPR
is
negatively
influenced
by
family
members
who
interfere
with
the
treatment.
In
particular,
a
conflict
between
staff
and
family
members
may
arise
when
they
have
a
different
opinion
about
what
is
the
right
thing
to
do,
to
keep
resuscitating
or
to
discontinue
it.
members
should
gener-
ally
be
offered
the
chance
to
be
present
during
CPR.
The
importance
of
informing
them
about
what
is
happening
and
caring
for
them
during
the
procedure
is
emphasised.
In
our
opinion,
the
emergency
team
members
have
a
professional
responsibility
to
provide
ini-
tial
emotional
support
for
the
people
who
have
lost
someone
close
to
them
before
leaving
the
scene.
They
should
also
help
them
to
contact
other
persons
or
organisations
that
can
offer
further
sup-
port.
Family
members
are
generally
satisfied
with
the
overall
care
provided
by
the
emergency
personnel
at
the
scene.
In
fact,
family
members
often
prefer
or
accept
that
CPR
is
terminated
at
home
so
that
their
dead
loved
ones
are
not
transported
to
hospital.
More-
over,
terminating
CPR
and
caring
for
the
patient’s
survivors
at
home
appear
to
have
a
positive
impact
on
the
grieving
8.
The
formulation
of
guidelines
that
deal
with
ethical
problems
related
to
out-of-hospital
CPR
Guidelines
cannot
possibly
cover
all
the
circumstances
that
surround
a
particular
situation.
As
a
result,
the
ambulance
per-
sonnel
always
have
to
use
their
knowledge,
skills,
experience
and
values
when
dealing
with
decisions
and
situations
related
to
out-of-
hospital
CPR.
Moreover,
there
are
two
important
things
that
must
be
accepted.
Firstly,
it
is
an
inevitable
fact
that
some
resuscitation

30
A.
Ågård
et
al.
/
Resuscitation
83 (2012) 27–
31
attempts
will
be
subsequently
considered
unethical
or
unjusti-
fied,
when
further
information
about
the
medical
condition
of
a
patient
prior
to
the
cardiac
arrest
is
obtained,
for
example.
Second,
guidelines
may
help
to
define
some
situations
in
which
it
might
be
justified
to
withhold
or
withdraw
CPR.
However,
when
there
is
the
slightest
doubt
about
what
is
the
right
thing
to
do,
the
active
treatment
strategy
should
be
chosen.
9.
Conclusion
Our
views
can
be
summarised
thus:
General
ethical
aspects
• The
overall
objective
of
CPR
is
to
restore
the
patient
to
a
life
of
(from
the
viewpoint
of
the
patient)
acceptable
quality,
if
this
is
what
the
patient
wants.
• A
successful
CPR
attempt
means
that
the
patient
can
be
dis-
charged
from
hospital
with
acceptable
quality
of
life
and
in
accordance
with
his
or
her
will.
• Decisions
to
withhold
or
withdraw
CPR
must
always
be
based
on
sufficient
information.
As
a
result,
it
is
important
to
accept
that
some
resuscitation
attempts
will
be
subsequently
regarded
as
unethical
or
unjustified,
when
further
information
about
the
medical
condition
of
a
patient
prior
to
the
cardiac
arrest
is
obtained.
• It
is
generally
beyond
the
competence
of
the
emergency
per-
sonnel
to
assess
whether
or
not
a
resuscitation
attempt
is
in
the
patient’s
best
interest,
or
to
determine
the
kind
of
death
the
patient
would
have
preferred.
As
a
result,
the
views
of
the
mem-
bers
of
the
emergency
team
regarding
what
constitutes
a
peaceful
and
dignified
death
should
be
used
very
cautiously
when
guiding
the
action
that
should
be
taken.
• There
is
no
relevant
ethical
difference
between
not
initiating
and
initiating
and
subsequently
withdrawing
CPR
from
the
patient’s
perspective,
as
the
consequence
is
basically
the
same
–
the
patient
will
die.
The
decision-making
process
• The
general
rule
is
to
initiate
CPR
when
confronted
by
a
person
with
an
out-of-hospital
cardiac
arrest.
As
a
result,
when
there
is
the
slightest
doubt
about
what
is
the
right
thing
to
do,
the
active
treatment
strategy
should
always
be
chosen.
• An
experienced
ambulance
or
emergency
services
staff
member
with
the
appropriate
training
could
be
given
a
mandate
to
decide
not
to
initiate
or
to
stop
a
resuscitation
attempt
in
well-defined
conditions.
• The
creation
of
an
organisation
in
which
emergency
personnel
can
easily
consult
physicians
with
a
particular
area
of
expertise
in
emergency
medicine
at
the
prehospital
stage,
to
obtain
support,
advice
or
a
second
opinion,
is
recommended.
• Family
members
could
be
asked
if
they
know,
or
what
they
think
the
patient
would
have
wanted,
when
it
comes
to
CPR.
However,
it
should
be
made
clear
to
them
that
they
are
not
responsible
for
the
final
decision.
• The
emergency
personnel
involved
in
a
resuscitation
attempt
outside
hospital
should
obtain
information
about
whether
or
not
the
patient
survived
to
be
discharged
from
hospital
and
about
his/her
mental
and
physical
condition
at
discharge.
Withholding
or
withdrawing
out-of-hospital
CPR
• A
decision
to
withhold
or
withdraw
CPR
should
be
made
after
weighing
the
relevant
medical
facts
and
ethical
aspects
in
the
concrete
situation.
The
potential
risk
of
severe
cerebral
damage
for
the
survivor,
as
well
as
the
patient’s
biological
age,
should
be
taken
into
account.
However,
chronological
age
per
se
should
not
be
used
as
a
single
discriminatory
factor
for
treatment
decisions
related
to
CPR.
• Treatment
with
CPR
for
an
out-of-hospital
cardiac
arrest
can
be
withheld
or
withdrawn
in
an
out-of-hospital
setting
in
obvious
cases
of
mortal
injury
or
death
(e.g.,
decapitation,
rigor
mortis
and
decomposition),
or
when
the
following
criteria
are
met:
the
arrest
was
not
witnessed;
no
bystander
cardiopulmonary
resuscitation
was
administered;
the
time
between
the
alarm
and
the
arrival
of
the
ambulance
exceeded
15
min;
and
the
type
of
arrhythmia
recorded
by
the
rescue
team
is
asystole
(Figure).
• Moreover,
in
cases
in
which
the
emergency
personnel
have
access
to
definite
and
reliable
information
that
the
patient
with
a
cardiac
arrest
is
suffering
from
the
end
stage
of
an
irreversible
medi-
cal
condition
(life
expectancy
<
6–12
months)
and
there
is
a
clear
written
statement
(an
advance
directive)
saying
that
he
or
she
does
not
want
CPR
and/or
a
valid
do
not
resuscitate
(DNR)
order,
treatment
with
CPR
could
be
withheld
or
withdrawn
in
an
out-
of-hospital
setting.
Caring
for
those
who
are
close
to
the
patient
and/or
bystanders
• Family
members
should
generally
be
offered
the
chance
to
be
present
during
CPR.
If
they
wish
to
be
present,
it
is
important
that
the
personnel
provide
information
about
what
is
happening
and
take
care
of
them
during
the
procedure.
• It
could
be
regarded
as
ethically
defensible
for
the
personnel
to
continue
CPR
for
a
short
period
time,
even
though
they
expect
it
to
be
unsuccessful,
to
show
bystanders/family
members
that
they
did
something
good
when
they
initiated
CPR
and
to
make
them
feel
that
everything
that
can
possibly
be
done
to
save
the
patient’s
life
is
actually
being
done.
• Before
leaving
the
scene,
emergency
team
members
have
a
pro-
fessional
responsibility
to
provide
initial
emotional
support
for
the
people
who
have
lost
someone
close
to
them.
Conflict
of
interest
statement
None
of
the
authors
has
a
conflict
of
interest.
References
1.
Lippert
FK,
Raffay
V,
Georgiou
M,
Steen
PA,
Bossaert
L.
European
Resuscitation
Council
guidelines
for
resuscitation
2010.
Section
10.
The
ethics
of
resuscitation
and
end-of-life
decisions.
Resuscitation
2010;81:1444–51.
2.
Morrison
LJ,
Kierzek
G,
Diekema
DS,
Sayre
MR,
Silvers
SM,
Mancini
ME.
Part
3.
Ethics:
2010
American
Heart
Association
guidelines
for
cardiopulmonary
resuscitation
and
emergency
cardiovascular
care.
Circulation
2010;122(Suppl.
3):S665–75.
3.
Decisions
relating
to
cardiopulmonary
resuscitation.
A
joint
statement
from
the
British
Medical
Association,
the
Resuscitation
Council
(UK)
and
the
Royal
College
of
Nursing,
2007.
4.
Sandman
L,
Nordmark
A.
Ethical
conflicts
in
prehospital
emergency
care.
Nurs
Ethics
2006;13:592–607.
5.
Marco
CA,
Schears
RM.
Prehospital
resuscitation
practices:
a
survey
of
prehos-
pital
providers.
J
Emerg
Med
2003;24:101–6.
6.
Mohr
M,
Kettler
D.
Ethical
aspects
of
prehospital
CPR.
Ann
Emerg
Med
1997;17:298–300.
7. Naess
A-C,
Steen
E,
Steen
PA.
Ethics
in
treatment
decisions
during
out-of-
hospital
resuscitation.
Resuscitation
1997;33:245–56.
8.
Bailey
ED,
Wydro
GC,
Cone
DC.
Termination
of
resuscitation
in
the
prehospital
setting
for
adult
patients
suffering
nontraumatic
cardiac
arrest.
National
Asso-
ciation
of
EMS
Physicians
Standards
and
Clinical
Practice
Committee.
Prehosp
Emerg
Care
2000;4:190–5.
9.
Morrison
LJ,
Verbeek
PR,
Vermeulen
MJ,
et
al.
Derivation
and
evaluation
of
a
termination
clinical
prediction
rule
for
advanced
life
support
providers.
Resus-
citation
2007;74:266–75.
10.
Macklin
R.
Dignity
is
a
useless
concept.
BMJ
2003;327:1419–20.
11.
Lo
B.
End-of-life
care
after
termination
of
SUPPORT.
Hastings
Cent
Rep
1995;25:S6–8.
12. Iserson
KV.
Foregoing
prehospital
care:
should
ambulance
staff
always
resusci-
tate.
J
Med
Ethics
1991;17:19–24.

A.
Ågård
et
al.
/
Resuscitation
83 (2012) 27–
31
31
13.
Melltorp
G,
Nilstun
T.
The
difference
between
withholding
and
withdrawing
life-sustaining
treatment.
Intensive
Care
Med
1997;23:1264–7.
14.
Bishai
D,
Siegel
A.
Moral
obligation
to
families
when
there
is
a
sudden
death.
J
Clin
Ethics
2001;12:382–7.
15.
Jaslow
D,
Barbara
JA,
Johnson
E,
Moore
W.
Termination
of
nontraumatic
car-
diac
arrest
resuscitative
efforts
in
the
field:
a
national
survey.
Acad
Emerg
Med
1997;4:904–7.
16. Compton
S,
Madgy
A,
Goldstein
M,
Sandhu,
Dunne
R,
Swor
R.
Emergency
medi-
cal
service
providers’
experience
with
family
presence
during
cardiopulmonary
resuscitation.
Resuscitation
2006;70:223–8.
17.
Delbridge
TR,
Fosnocht
DE,
Garrison
HG,
Auble
TE.
Field
termination
of
unsuccessful
out-of-hospital
cardiac
arrest
resuscitation:
acceptance
by
family
members.
Ann
Emerg
Med
1996;27:649–54.
18.
Schmidt
TA,
Harrahill
MA.
Family
response
to
out-of-hospital
death.
Acad
Emerg
Med
1995;2:513–8.
19.
Edwardsen
EA,
Chiumento
S,
Davis
E.
Family
perspective
of
medical
care
and
grief
support
after
field
termination
by
emergency
medical
services
personnel:
a
preliminary
report.
Prehosp
Emerg
Care
2002;6:
440–4.
Document Outline
- Guidance for ambulance personnel on decisions and situations related to out-of-hospital CPR
- 1 Introduction
- 2 The objective of CPR
- 3 Choices to be made
- 4 Attempting to act in the patient's best interest
- 5 Advance directives
- 6 Withholding or withdrawing CPR
- 7 The presence of family members and bystanders
- 8 The formulation of guidelines that deal with ethical problems related to out-of-hospital CPR
- 9 Conclusion
- Conflict of interest statement
- References
Wyszukiwarka
Podobne podstrony:
Guidance for ambulance personnel on decisions and situations related to out-of-hospital CPR, MEDYCYN
Effect of?renaline on survival in out of hospital?rdiac arrest
20130829B Quick Facts and Terminology Related to the End Times
Historic Dates and Events Related to Vaccines and Immunization
Norris, C E i Colman, A M (1993) Context effects on memory for televiosion advertisements Social Bah
5 The importance of memory and personality on students' success
Installing LAMP On Ubuntu For Newbies, HowtoForge Linux Howtos and Tutorials
Accounting Recording and Firm Reporting as Source of Information for Users to Take Economic Decision
139167632 Meyer Schapiro The Still Life as a Personal Object A Note on Heidegger and Van Gogh
Fact and Value = Essays on Ethics and Metaphysics for Judith Jarvis Thomson (MIT 2001)
Herbs for Sports Performance, Energy and Recovery Guide to Optimal Sports Nutrition
5th Fábos Conference on Landscape and Greenway Planning 2016
[30]Dietary flavonoids effects on xenobiotic and carcinogen metabolism
53 755 765 Effect of Microstructural Homogenity on Mechanical and Thermal Fatique
Zizek on Deleuze and Lacan
Langtry Popper on Induction and Independence
RATIONALITY AND SITUATIONAL LOGIC IN POPPER
więcej podobnych podstron